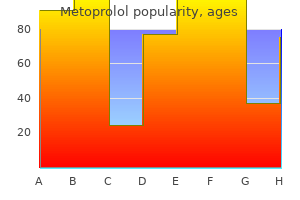
Metoprolol dosages: 100 mg, 50 mg, 25 mg, 12.5 mg
Metoprolol packs: 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills, 30 pills
Generic metoprolol 100 mg with visa
Variant process or approaches: Endoscopic approaches are being developed for a quantity of fracture sites. Resorbable plates and screws, particularly for pediatric cases, can be utilized through the identical surgical approaches. Panfacial fracture treatment protocol, based on reconstructing load-bearing structures of the facial skeleton. A: Projection of the midface is created by reconstructing the zygomatic arches, ranging from the secure a half of the temporal bone. B: the zygomas are fastened to the arches and to the frontal bone to create the ultimate projection of the midface. C: the width of the midface is reconstructed by repositioning the central midface (orbits and nose) to its correct position, in relation to the zygomas and frontal bone. Concomitantly, canthopexy is fixed, and the frontal bone and sinus fractures are handled. C: LeFort I is a horizontal fracture involving mobilization of dentition and maxilla. A: Anatomic areas of the mandible and B: frequency of fractures in these areas. Standard anesthesia and surgical setup for a maxillofacial surgical process and certain craniofacial surgical procedures. The table could additionally be rotated 90��180� with anesthesia gear and personnel on the foot or off to one aspect. When unsure, a tracheostomy under native anesthesia or awake intubation should be thought-about. In malar or nasal bone fractures, the fixation could additionally be precarious, making it undesirable to use masks ventilation on the termination of the procedure and necessitating awake extubation. Facial nerve monitoring could also be required, contraindicating the utilization of muscle relaxants. The cause of restricted mouth opening should be decided earlier than induction of anesthesia. Often, the airway can be managed simply by inserting an oropharyngeal airway; failing this, an emergency intubation will be needed. Emergency oral intubation may be sophisticated by an unstable C-spine and restricted jaw opening, along with blood and particles in the oropharynx, making visualization tough if not unimaginable. As with any trauma sufferer, attention is first directed towards maintaining the airway and restoration of fluid quantity. In the case of facial trauma, nevertheless, intubation of the trachea may be impossible. Fischer K, et al: Injuries associated with mandible fractures sustained in motorcar collisions. The commonest is the LeFort I, a transverse osteotomy, above the apices of the enamel, used to right maxillary retrusion or maxillary vertical excess or deficiency. One of the targets in reaching improved perform is to improve the occlusion, as categorised by Angle. An intraoral vestibular incision is used for this approach, adopted by an osteotomy of the maxilla, with both a burr or a saw, and accomplished with osteotomes. Further interdental osteotomies creating a quantity of maxillary segments could additionally be required. With maxillary advancements, iliac or cranial bone grafts are often essential to shut the bony hole created. The key relationships to be discerned are those of the first molar enamel, cuspids, and incisors. Zellin G, Rasmusson L, P�lsson J, et al: Evaluation of hemorrhage depressors on blood loss throughout orthognathic surgical procedure: a retrospective research. Surgical correction of the essential mandibular deformity entails either advancing or retruding the mandible. The most typical process for that is the sagittal ramus break up osteotomy (Obwegeser;. The mandible is split with the inferior alveolar nerve solely throughout the anterior segment, such that the tooth-bearing anterior segment can slide forward or backward to appropriate the unique deformity. A number of other strategies of mandibular osteotomies exist, often involving the ramus area of the mandible, and are carried out through an intraoral approach. A, B: "J" stripper used to take away muscle attachments from medial aspect of distal segment.
Order metoprolol no prescription
After a Betadine prep, anesthetic eye drops are used, adopted by the insertion of protecting corneal shields. The treatment then begins with one or more passes performed at numerous vitality levels. Usual preop prognosis: Wrinkles, precancerous skin lesions (actinic keratoses), acne scars, and traumatic scars. All dental caries are removed, the restorations are positioned, and all particles is irrigated and suctioned away from the rubber dam, which is then eliminated. After the operative phase of treatment is completed, the subsequent treatment phases proceed. After the remedy is completed, the dentist examines the mouth and removes any free gauze, debris, or other materials left over from the therapy earlier than the anesthesiologist begins the process of emergence from anesthesia. Examples embody a 20-mo-old child with early childhood caries, an 8-yrold autistic youngster, or a baby of any age with cerebral palsy, obesity, Down syndrome, or other congenital syndrome. These patients must be screened upfront for scientific situations that might put them at risk for problems intraop or postop. Specifically, a patient with any cardiac, respiratory, endocrine, or neurologic downside should be evaluated. Examples of such circumstances embody gentle nonsteroid-dependent asthma, corrected congenital coronary heart disease, or a stable Sz dysfunction. Following sedation, the patient is positioned in the dental chair, with the pinnacle positioned to maintain an open airway. A nasal airway is positioned with care (to avoid epistaxis) after the dental x-rays are taken. The anesthesiologist must be continually vigilant in maintaining an open airway in these patients in the face of an oral procedure. Dental implants are inserted surgically into the mandibular or maxillary alveolar bone the place tooth are missing. Single implants may be done with native anesthesia, but a number of or advanced procedures are finest achieved with iv sedation. After the local anesthetic is administered, a mucoperiosteal flap is raised over the edentulous alveolus, and the bone is exposed. Precise drill holes are made in the bone, and the implants are screwed or tapped into place. Bone grafting could additionally be necessary around the implants to fill in defects and is carried out using autologous, allogenic, xenogenic, or synthetic materials. The bone is allowed to heal around the implant, and 2-6 mo later the implant can be utilized to attach crowns, bridges, or dentures. Most minor grafting procedures are completed in the dental workplace underneath iv sedation and native anesthesia. The anesthesiologist ought to be consulted in advance about these patients so that questions on their medical circumstances could be answered and a present record of medicines can be obtained. If chronic medical circumstances are stable, patients often can obtain "aware sedation" and monitoring by the anesthesiologist for this process within the office. In the adult affected person having dental implants, the upkeep of a flippantly sedated state is achieved using a combination of iv midazolam, fentanyl (or meperidine), and small quantities of ketamine (20�30 mg/dose). Dexamethasone 8 mg and metoclopramide 15 mg are useful as an antiemetic mixture. It may be given, however, in small doses to the affected person who requires greater than the opposite medicine for sedation. Adult bougie 15 Fr handed through incision with coude tip directed caudally attempting to feel for tracheal clicks and/or carinal hang-up sign. Because of the excessive intrapericardial pressures, all "filling pressures" of each proper and left heart appear excessive when preload is actually very low. Precepted hands-on training must be sought prior to using ultrasound for analysis or therapy of cardiac tamponade. Once diagnosis of cardiac tamponade is made, elevate head of bed to 30�45� to allow gravity to help in fluid entry. An 18 g spinal needle is directed in the direction of the left shoulder and inserted at a 45� angle to the pores and skin.
Purchase metoprolol 100mg mastercard
A scan is initially carried out within the sagittal orientation at the superior medial border of the scapula to identify the pleura at roughly 4 cm. By transferring the ultrasound transducer cephalad, the suprascapular fossa is recognized. While the supraspinatus muscle and the bony fossa beneath are being imaged, the ultrasound transducer is moved slowly laterally to find the suprascapular notch [26�30]. A 21-gauge, 50 mm B-bevel needle is inserted alongside the longitudinal axis of the ultrasound beam about 1 cm away from the medial border of the probe. The needle is visualized in its full course; the end level for injection is an ultrasound picture demonstrating the needle tip in proximity to the suprascapular nerve in the suprascapular notch. Color Doppler is used to visualize the suprascapular vessels and to keep away from contacting them. The injection is done under real-time ultrasound steerage to be sure that the needle is underneath the coracoclavicular ligament and to visualize unfold. A decrease quantity of 5 cc has been beneficial with an ultrasound approach to avoid unfold to the brachial plexus. There should be minimal resistance to injection; however a paresthesia throughout injection could additionally be commonly encountered. Another proximal strategy focusing on the suprascapular nerve somewhat than the notch has additionally been described [27, 31]. The affected person is within the sitting position with the shoulder in a neutral place with the hand resting on the ipsilateral thigh. The lateral and inferior cutaneous space of the neck is cleaned, and an ultrasound transducer is utilized to the facet of the neck at the degree of the cricoid cartilage in a transverse oblique aircraft to obtain the most effective view of the brachial plexus. The transducer is oriented in the oblique sagittal aircraft, and the hand of the operator is resting on the clavicle. The shoulder joint is in neutral place and the hand of the volunteer is resting on the thigh to visualize the trapezius muscle in transverse part, the inferior stomach of the omohyoid muscle within the longitudinal part, and the higher a half of the serratus anterior muscle under the omohyoid muscle. The suprascapular nerve is positioned within the fascia layer between the omohyoid muscle and the serratus anterior muscle. The needle is positioned in plane to the ultrasound probe, and 5 cc quantity of local anesthetic is injected with real-time ultrasound imaging. The patient is positioned in a inclined place with the hand both by the facet or beneath the pinnacle. The process is finished beneath fluoroscopic or ultrasound steerage as mentioned above. The position is confirmed by dye unfold and appropriate motor response of the supraspinatus and infraspinatus muscle tissue at 2 Hz stimulation. Sensory response is elicited as a paresthesia to the posterior and superior a part of the shoulder with 50 Hz stimulation at zero. The radiofrequency probe is inserted and connected to the radiofrequency generator. Precautions Suprascapular nerve block is an easy process to perform and a secure approach for offering ache relief from various forms of shoulder accidents [32]. Suprascapular nerve block permits long-lasting, efficient analgesia for numerous situations affecting the shoulder similar to rheumatologic disorders, trauma, and postoperative and most cancers ache. Posterior, superior, and anterior approaches are used, with posterior being the most typical. Pneumothorax and nerve injury are the two most dreaded issues of suprascapular nerve block. Ultrasound can function a device to reduce problems, although this has not proven to be the case for different ultrasound assisted nerve blocks. Neuromodulation using peripheral stimulators and pulsed radiofrequency shall be used more generally for long-term management of shoulder pain [33]. Further analysis is required to better identity the specific shoulder pathologic illnesses which is able to respond positively to a suprascapular nerve block [34]. The nerve could also be accessed either by classic posterior method utilizing the suprascapular notch as an important landmark or by the anterior approach which requires using ultrasound. In an acute setting within the perioperative interval, suprascapular block together with axillary block could also be a viable different to interscalene block especially in a patient with lung illness. Pneumothorax is essentially the most dreaded complication which may be averted with careful approach and presumably with the usage of ultrasound with dynamic visualization of the needle.
Buy metoprolol on line
Facet joint ache in chronic spinal ache: an analysis of prevalence and false-positive rate of diagnostic blocks. Research designs in interventional pain administration: is randomization superior, desirable or important Parameters in electrode positioning in thoracic percutaneous facet denervation: an anatomical research. The treatment of persistent thoracic segmental ache by radiofrequency percutaneous partial rhizotomy. Electrode positioning in thoracic percutaneous partial rhizotomy: an anatomical study. Thoracic zygapophyseal pain: a evaluate and description of an intraarticular block method. Classification of continual ache: descriptions of continual ache syndromes and definitions of ache phrases. The lumbosacral articulation: a proof of many cases of lumbago, sciatica, and paraplegia. Pain administration by radiofrequency procedures in the cervical and thoracic spine: a clinical and anatomical study. The nerve provide of the vertebral column and its related buildings in the monkey. Study of Pain, the prevalence of thoracic side joint pain has been decided to be 34�48%. To keep the validity of diagnostic blocks, both comparative native anesthetic blocks or placebocontrolled blocks must be carried out as a result of single blocks carry a false-positive rate of 42�58%. Multiple modalities are available for managing thoracic aspect joint pain, together with intra-articular injections, medial branch blocks, and radiofrequency neurotomy. Adequate training and experience, proper technique, meticulous adherence to safety pointers, and highquality fluoroscopic imaging gear are needed prerequisites for the protected and effective injecting of thoracic buildings. A best-evidence systematic appraisal of the diagnostic accuracy and utility of side (zygapophysial) joint injections in persistent spinal pain. Identification of prostaglandin E2 and leukotriene B4 within the synovial fluid of painful, dysfunctional temporomandibular joints. Rat model of lumbar aspect joint osteoarthritis associated with facet-mediated mechanical hyperalgesia induced by intra-articular injection of monosodium iodoacetate. Lumbar side joint compressive damage induces lasting changes in local construction, nociceptive scores and inflammatory mediators in a novel rat model. The function of thoracic medial department blocks in managing persistent mid and higher back pain: a randomized, double-blind, active-control trial with a 2-year follow-up. Evaluation of therapeutic thoracic medial branch block effectiveness in persistent thoracic pain: a prospective consequence study with minimal 1-year follow up. Outcomes of percutaneous zygapophysial and sacroiliac joint neurotomy in a neighborhood setting. The utility of comparative local anesthetic blocks versus placebo-controlled blocks for the diagnosis of cervical zygapophysial joint ache. Comparative local anesthetic blocks in the analysis of cervical zygapophysial joints pain. Evaluation of effect of sedation as a confounding issue within the diagnostic validity of lumbar side joint ache: a potential, randomized, double-blind, placebocontrolled analysis. International spinal injection society guidelines for the performance of spinal injection procedures. In: Radiofrequency part 2: thoracic and cervical region, headache and facial ache. Topographic anatomy of the posterior ramus of thoracic spinal nerve and surrounding buildings. The vascular provide to the spinal wire and its relationship to anterior backbone surgical approaches. Medial department neurotomy in management of persistent spinal pain: systematic evaluate of the proof. Percutaneous radiofrequency facet rhizotomy-experience with 118 procedures and reappraisal of its value. Regional anaesthesia and antithrombotic 20 Thoracic Facet Joint Interventions agents: recommendations of the European society of anaesthesiology. Periprocedural anticoagulation � adult � inpatient and ambulatory� clinical apply guideline. Falco, and Vijay Singh 21 Introduction Chronic neck ache within the basic inhabitants with or with out sprain or injury is common.
Order 50 mg metoprolol mastercard
Growth of spinal interventional pain administration strategies: evaluation of utilization developments and Medicare expenditures 2000 to 2008. Cohen 2 Introduction Pain Signaling Transduction, transmission, modulation, and perception are the core components concerned in the mechanisms of pain physiology. These parts collectively comprise the pathway from the onset of pain on the time of preliminary tissue harm to its ultimate processing within the mind. Neuropathic ache is exclusive in that it bypasses the first step of changing a stimulus to an electrical impulse, as the stimulus involves direct injury to the nerve. Together, nociceptive ache and neuropathic ache form the acute ends of a "continuum of ache," alongside which every mechanism remains to be not fully understood (Table 2. Yet for clinicians, identification of the mechanisms of ache is critically important for effective management, as it informs therapy selections at every step. It is broadly acknowledged that mechanism-based pain treatment is theoretically superior to illness or etiologic-based treatment, although in medical follow that is troublesome to implement [2, 3]. Since ache includes the whole nervous system, it is important to perceive the individual parts along which the signals journey. Transduction is the process of converting a noxious stimulation from tissue harm to a nociceptive sign. Finally, perception is the interpretation of the sign by cognitive and emotional responses in the mind, which considers context, previous experiences, and expectations. From an evolutionary perspective, this sequence was meant to defend towards additional harm; however, given the lengthy cascade of biological occasions that transpire, maladaptation at any of the points alongside the chain may find yourself in pathological pain. Cohen Aching, throbbing, dull, strain Uncommon Pain-induced weakness Radiation Exacerbations Autonomic changes Distal, usually in dermatomal distribution Common and unpredictable Color or temperature modifications, swelling, or sudomotor exercise May have hypersensitivity in instant vicinity of tissue injury. Ligand-gated ion channel receptors operate by activating ion channels or second messenger techniques. Once activated by the ligand, second messenger techniques act by way of phospholipase-linked or adenylate cyclase-linked receptors to open ion channels throughout the cell membrane and initiate an motion potential. Data from Cohen and Mao [1] Transmission Nerve Fibers There are three major nerve courses involved in pain transmission: A�, A, and C afferent nerves. These nerves could be associated with mechanical nociceptors, mechanothermal nociceptors, and polymodal nociceptors, which respond to mechanical, chemical, and thermal noxious stimuli. Among the three sorts, the C afferent nerves are the smallest in diameter and are unmyelinated. These C nerves direct indicators from visceral, thermal, autonomic, and polymodal nociceptors. Neuronal fibers from the A nerves terminate in free nociceptor endings, as properly as partially encapsulated nociceptive terminals. These nerve fibers usually terminate in encapsulated nonnociceptive endings, corresponding to Pacinian corpuscles and Transduction Nociceptors the basic unit of step one along the pathway � transduction � is the nociceptor. These specialised neurons are sensitive to three kinds of injurious stimuli � mechanical, thermal, and chemical � and are repeatedly communicating with immune, inflammatory, vascular, and local cells to reply to any modifications in tissue chemistry, extracellular matrix, and other neuronal, endocrine, or systemic byproducts. Voltage-gated ion channels, ligand-gated ion channels, and ligand-mediated second messenger mechanisms facilitate detection of the noxious stimuli. Voltage-gated ion channels enable the influx of sodium and calcium ions, which at a certain threshold will generate an motion potential that can relay the pain signal more proximally in the nervous system. After propagation of the impulse, an efflux of potassium ions through the channels enables the neurons to repolarize to their resting state. Under regular situations, A nerves predominantly convey signals of light contact and stress, however not ache. However in pathological circumstances, they might bear a phenotypic switch and acquire the capacity to enhance the excitability of spinal cord nociceptive neurons. Within afferent nerves lie two types of cutaneous nociceptive fibers, A and C fibers. Intuitively, A fibers are situated throughout the A and A afferent nerves, whereas C fibers lie within C nerves.
Cheap metoprolol generic
The spindle-shaped cells are variably optimistic for endothelial cell markers and could also be focally constructive for actin. In some cases morbidity and mortality are associated with problems arising from the tumor because of its destructive and infiltrative growth. Retroperitoneal tumors are normally related to intestinal obstruction and jaundice. A frequent affiliation with these tumors at almost any web site is Kasabach-Merritt syndrome. These lesions could additionally be hard to resect correctly (because of their anatomic location), but plainly true recurrence is infrequent. Rare perinodal or nodal metastasis has been described,240 but distant metastasis has not been reported to date. A shut affiliation between tufted angioma and kaposiform hemangioendothelioma has been advised on the premise of scientific and histologic overlap and the truth that each situations might induce Kasabach-Merritt syndrome. Infantile capillary hemangioma ("juvenile hemangioendothelioma"; see later discussion) consists of solid nodules of incompletely canalized capillaries without a spindle cell component. Kaposiform hemangioendothelioma can be distinguished from angiosarcoma by its lack of cytologic atypia and the absence of individually infiltrative, anastomosing channels. It presents as a slowly rising cutaneous tumor, most frequently in younger adults; no sex predominance is seen. Very hardly ever, these lesions can come up after radiotherapy or in the setting of chronic lymphedema. This appearance is conferred by the presence of elongated, arborizing blood vessels. A outstanding stromal and intraluminal lymphocytic infiltrate is present in maybe 50% of circumstances. These endothelial cells have restricted, normally basal, cytoplasm, and vacuolation is rare. The vascular lumina might contain occasional papillae with hyaline collagenous cores. Most tumors present focally stable areas composed of monomorphic spindle or epithelioid cells, which normally stain positively for endothelial markers. Recently, nonetheless, follow-up in eight of 12 reported cases revealed neither native recurrences nor metastatic spread. Therefore the problem about the true malignant potential of this tumor will stay unsolved till further collection are reported. Hobnail hemangioma happens primarily in kids and younger adults and in a extensive range of anatomic sites, including the oral cavity. Histologically, the lesions are most likely to be superficial and circumscribed, with a sparse inflammatory infiltrate and only focal hobnail endothelial cells. Angiosarcoma normally happens in a unique medical setting and is characterized by irregularly infiltrative vascular channels, lined by atypical endothelial cells, which usually present multilayering. Histologic Appearances Using stringent diagnostic criteria, our experience and that of others255 recommend that these tumors are usually composed of dilated, irregular vascular channels resembling a cavernous lymphangioma, although some instances have smaller, irregularly branching vascular channels. Numerous lymphocytes are seen not solely in the surrounding stroma but in addition throughout the vascular channels. The endothelial cells lining a few of the spaces have a prominent atypical nucleus and inconspicuous cytoplasm, giving a typical hobnail or matchstick appearance. Most attribute is the presence of distinguished endothelial intraluminal papillary tufts. These hyaline cores seem to be composed of basement membrane material synthesized by the tumor cells. More than 50% of sufferers have a number of nodules, usually involving multiple tissue planes in the identical basic anatomic region-most often pores and skin, subcutis, and skeletal muscle and less typically bone. Despite this very worrisome presentation, metastasis seems to be very rare.
Order 12.5mg metoprolol with visa
An openapproach will utilize a transcolumellar incision to enable elevation of a nasal skin flap and degloving of the lower alar cartilages for direct and broad publicity of the nasal framework. Closed approaches use intercartilaginous, intracartilaginous, infracartilaginous, rim, hemitransfixion, and transfixion incisions (all hidden within the nose). The dorsum may be decreased utilizing a scalpel and/or rasps beneath the undermined dorsal pores and skin and periosteum. The septum is addressed as necessary through a hemitransfixion incision (� cartilage harvest). Tip reduction by scalpel or scissor resection of the decrease alar cartilage � tip suture is subsequent. Nasal osteotomies with an osteotome and mallet begin at the base of the nasal bones alongside the piriform aperture. Access factors for the osteotomies could be intranasally, externally, or via an intraoral vestibular incision. Digital manipulation completes the fractures, and this is when most of the blood loss happens. Dorsal and tip grafts are applied as essential, with alar modifications made final. Alar reduction entails wedge resection of the lateral alar base and primary closure. B: Delivery strategy, utilizing a high intercartilaginous incision and a marginal incision to facilitate delivery of the lateral crura. Rhinoplasty Techniques Depending on the kind of rhinoplasty performed, totally different dressings will be utilized at the finish of the procedure. When nasal bone osteotomies are used, the affected person will require a dorsal nasal splint � bilateral nasal packing. When septal manipulation is needed, nasal packing or some kind of septal splint may be placed. The packs are usually removed within 3 d, however the splints could be maintained for much longer and the nasal airways saved patent with vasoconstrictor nasal sprays. Variant procedures or approaches: Placement of a columellar strut (cartilage graft) and release of the tip depressor muscle often are achieved through intraoral vestibular incisions (behind the higher lip). Molliex S, Navez M, Baylot D, et al: Regional anaesthesia for outpatient nasal surgery. It is used widely for the periorbital and perioral creases and wrinkles not addressed by beforehand described facial beauty surgical methods. The choice of anesthetic depends extra on the particular surgical procedures to be carried out first, because the laser process is usually adjunctive and added on the finish. Facial laser resurfacing is done frequently in an office-based setting (see Chapter 14. Everyone current, together with the patient and all medical personnel, requires laser-specific. Protection for the affected person and medical personnel is offered by: Utilizing a smoke evacuation system 2 cm from created plume Wearing high-filtration masks. Note that these masks turn into less effective if moistened from perspiration throughout an extended case; if the laser is to be used at the end of a case, altering masks before using the laser may be prudent. Facial Plastic Surgery Clinics of North America: Management of anesthesia and facility in facelift surgery. Suggested Viewing Links are available online to the next movies: Live Surgery Split Thickness Skin Graft. The patient is positioned both with the arms kidnapped at 90� or with the arms tucked at the sides. Local anesthetic (� epinephrine) is infiltrated into the pores and skin at the incision web site and underneath the glandular tissue. Implant insertion may be accomplished through inframammary, periareolar, transaxillary, or transumbilical incisions. When the implant is placed in the submuscular position, the pectoralis muscle is split from its insertion along the inframammary fold and typically along the sternal insertion to enable the muscle to drape over the implant. Regardless of the location of the pocket, the surgical wound is carefully irrigated and inspected for hemostasis. Sizers, either predetermined volumes of silicone gel or adjustable saline- or air-filled temporary implants, could also be used to assist decide the appropriate ultimate volume and placement.
Real Experiences: Customer Reviews on Metoprolol
Mojok, 63 years: Recently with the arrival of markers of lymphatic endothelium, an try has been made to elucidate line of differentiation.
Kurt, 53 years: In the first stage (A-C), bilateral straight line repairs are accomplished after the prolabium is split vertically into three forks.
Masil, 35 years: After the skin has been closed, the location of the nipple and areola is marked and excised, and the nippleareola advanced is delivered and sutured into position.
Onatas, 64 years: Cup the inverted fundus within the palm of the hand, elevate the inverted prolapsed fundus.
Giores, 42 years: The result could be bothersome stress urinary incontinence and/or incomplete emptying for the patient (see Operations for Stress Urinary Incontinence, p.
Kayor, 40 years: Up to 15% of gnathic lesions will recur,129 however sinonasal tract lesions are less prone to recur after curettage.
Givess, 55 years: Here the uterosacral ligaments are plicated and sutured collectively in the midline, at the level of the pouch of Douglas, to obliterate that space.
10 of 10 - Review by J. Ernesto
Votes: 53 votes
Total customer reviews: 53