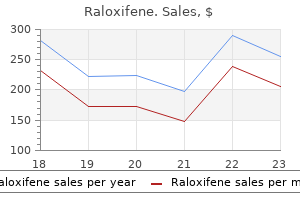
Raloxifene dosages: 60 mg
Raloxifene packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

Purchase raloxifene without prescription
These factors include medical comorbid circumstances, risk of recurrence, bowel function (fecal incontinence and constipation), diploma of prolapse, and presence of associated pelvic issues. Regardless of strategy, the goals of any prolapse surgery are to treat the prolapse and to tackle associated constipation or incontinence. Procedures for rectal prolapse can be classified into two major classes: perineal and transabdominal repairs. Perineal repairs are much less invasive, cause less perioperative pain and morbidity, and are related to lowered lengths of keep. They are favored for frail, elderly patients, but at some establishments, perineal repairs are favored for healthy sufferers, too. This strategy does carry a threat of an infection and issues related to the suture line or wound. In addition, the perineal approach is thought for recurrence charges which would possibly be four occasions higher than those of transabdominal operations; thus, the abdominal strategy is favored for medically fit patients who may tolerate this operation. A transabdominal restore requires basic anesthesia and should have extra devastating complications corresponding to anastomotic leak, abdominal sepsis, stricture, and adhesions. The introduction of minimally invasive approaches for the rationale that Nineties has added a new dimension to transabdominal prolapse surgical procedure and has been proven to cut back postoperative convalescence, making this approach more appealing. Our preference for all repairs is to have sufferers undergo full mechanical bowel preparation. We give perioperative intravenous antibiotics based on Surgical Care Improvement Project tips to provide prophylaxis towards enteric flora. All patients have a Foley catheter in place for bladder drainage and pneumatic compression stockings throughout surgery. Perineal Repairs Mucosal Sleeve Resection (Delorme Procedure) Although the mucosal sleeve resection was first described in 1900, it was not commonly used until Uhlig and Sullivan reported their expertise in 1979. We favor to perform the operation with the patient in the Kraske position; nonetheless, it may also be done in lithotomy place. After positioning the patient, the perineum and vagina are ready with an aseptic resolution. Other Nonsurgical Options for Prolapse No studies exist that examine operative repair with nonoperative therapy for rectal prolapse, nor are there definitive nonoperative alternate options to appropriate this condition. Notice that the rectal wall is plicated with sutures in an accordion-type trend and is located above the anal sphincters. The incision goes via the mucosa and submucosa initially, stripping this tube from the underlying inner anal sphincter and, more proximally, from the rectal muscular cuff. The operation commences by injecting 1:one hundred,000 epinephrine answer circumferentially into the submucosal aircraft just proximal to the dentate line. Once this plane is started, the free edge of mucosa and submucosa is tagged with sutures for ease in dealing with and in creating traction for simpler dissection. Continuing in a circumferential direction and using liberal quantities of injectable saline within the airplane between the submucosa and the muscular cuff, scissors are used to divide the attachments (we prefer fistula scissors) and to deliver the submucosa and mucosal cuff out of the rectum and anus. Penetrating blood vessels encountered during the dissection could be handled with electrocoagulation. It is important to keep strict hemostasis through the dissection to keep away from hematomas after the procedure. During this phase of the operation, we use copious amounts of antibiotic solution such as tetracycline to irrigate the surgical field. After the dissection is completed, the rectal muscle is plicated with suture such as no. The dissected mucosa is excised and the proximal line of resection is approximated to the distal incision line. Prolapse recurrence after the Delorme process varies from 10% to 15% in numerous collection. The procedure is nicely tolerated in high-risk patients however still carries a danger for issues of bleeding, urinary retention, and fecal impaction in as a lot as 12% of patients. In common, constipation and fecal incontinence tend to improve after surgery, the latter maybe because of the rectal muscular wall plication that creates a cumbersome, donut-like circumferential mass around the upper anal canal.
Discount 60mg raloxifene with mastercard
He reported that abnormally thick placentas had been more frequent in tall and overweight mothers, moms with diabetes, and in instances of fetal progress restriction and stillbirth. Placental thickness within the regular placenta tends to be uniform, according to a uniform intrauterine surroundings and equally permissive of villous arborization. Maternal uteroplacental pathology is related to reduced placental thickness because of decreased villous growth27,44 and with decreased placental vascular progress issue levels. The push and pull of growth-promoting and growth-limiting factors can be performed out within the growth of markedly variable placental thickness. As with giant and smaller diameters, a single measure of placental thickness within the diabetic placenta, at risk for marked variability for Location of Umbilical Cord Insertion Site Relative to the Edge of the Placental Disk Naeye34 also described antecedents to the development of marginal and velamentous umbilical cord insertions. Marginal twine insertion was associated with maternal acetonuria during the first trimester, diabetes mellitus, twins, main fetal malformations, placental development retardation, and erratically accelerated villus maturation. Antecedents for the event of velamentous wire insertion included maternal smoking, diabetes mellitus, congenital fetal syndromes, and placenta growth retardation. Of interest, velamentous twine insertion was associated with preterm birth and increased threat of neurological abnormalities at seven years, particularly hyperactivity syndromes. At birth, each marginal and velamentous umbilical cords are mechanically weak. Velamentous umbilical twine insertion is mechanically vulnerable even earlier than the membrane rupture because of elevated danger of umbilical twine and/or chorionic vessel mechanical compromise. This is as a outcome of of their location on the firm myometrial surface somewhat than the chorionic plate, inflated by the normally gentle maternal intervillous perfusion. After adjusting for the effects of different placental measures, increasing placental thickness has a adverse impact on birth weight for a given placental weight. We have discovered that the placental thickness�birth weight relationship is monotonic and optimistic in slope until placental thickness approaches four cm. After this, whereas placental weight continues to rise and placental thickness increases, the anticipated start weight drops precipitously. Abnormally low fetal weight for placental weight is attribute of both obesity46 and even in comparatively mild (diet-controlled) gestational diabetes. Naeye advised that when the placenta is large in the context of diabetes mellitus, the placental villi are histologically abnormally giant, quite than merely swollen by edema. As mentioned briefly earlier, in a big examine of 1472 consecutive singleton pregnancies with gestational diabetes, an abnormal fetal to placental weight ratio was present in four hundred (27. The irregular ratio resulted from increased placental weight somewhat than the decreased delivery weight. After adjusting for the effects of preterm delivery and vaginal delivery, an abnormal fetal to placental weight ratio was still related to a low Apgar rating, respiratory problems, and therapy for an infection. Lesions that may be interpreted as chronic fetal hypoxia in the comparatively bigger placentas of instances of gestational diabetes compared to controls. Univariate nonparametric correlations confirmed important optimistic relationships among and prepregnancy diabetes (r = 0. The contrast of our findings with those described earlier might level to a difference in the underlying maternal disease in the 1950�1960s compared to the final decade, however confirms the contribution of maternal metabolic pathology on the early (fractal) growth of the placenta previous to mid-gestation. Because both gestational age and abnormal form are related to thinner placentas, partial correlations that adjusted for these elements have been performed. The correlations of altered with disk thickness had been either unchanged (relative variability in disk thickness, r = zero. These observations are according to observations that irregular placental morphometry of placental change floor in even circumstances of gentle hyperglycemia. Recent epigenetic research suggest a direct impact of gestational exposure to diabetes on epigenetic modifications thought-about to result in lifelong illness risks. We have beforehand introduced a categorization scheme that classified histopathology lesions into the next major histopathology types. Maternal neutrophils are recruited from the decidual maternal spiral artery vasculature, the maternal neutrophils circulating in the blood perfusing the intervillous area, and fetal neutrophils are recruited from the fetal arteries and veins of the umbilical twine and chorionic plate.
Purchase cheap raloxifene on-line
Other authors have instructed that dysfunctional voiding may result from voluntary withholding of urination in people who work lengthy hours. Contraction of the pelvic floor-external sphincter advanced is a normal response to control urgent urination and results in a reflex inhibition of the detrusor. When this turns into recurring over time, the abnormal incoordination carries over to voluntary voiding, resulting in an intermittent urinary stream and residual urine. Usually a combination of behavioral, cognitive, and pharmacological therapies can used to obtain this. Fluoroscopic image taken throughout voiding shows a spinning high urethra with obstruction on the degree of the external sphincter. There is an elevated incidence of dysfunctional voiding in sexual abuse victims, and it has been linked to psychological stressors and elevated Hamilton scores measuring stress and nervousness; therefore, sure people might profit from mental well being therapy and help as nicely. Some pharmacotheraputic choices have been shown to be useful in patients with dysfunctional voiding. Several clinicians, including ourselves, have had anecdotal success with amitriptyline. Vaginal benzodiazepine suppositories even have been used as an adjunct remedy in high-tone pelvic flooring dysfunction related to dyspareunia. Finally, the role of neuromodulation in nonobstructive urinary retention has been shown to be helpful. There was a lower in the number of catheterizations by 50% and a lower in catheterized quantity from 379 to 109 mL. There was evidence of medical success in 58% and 71% of patients respectively at 5 years after implantation. Many of these women have a history or findings in preserving with polycystic ovary, which means that the abnormal sphincter could also be underneath the affect of estrogen and could be due to a hormone-sensitive channelopathy confined to the urethral sphincter; nevertheless, the precise pathophysiology of the disease is still unknown. Many of those girls often have a set off corresponding to basic anesthesia, urinary tract an infection, gynecologic surgical procedure, or childbirth. Oral agents and sphincteric Botox injections have been attempted with equivocal outcomes and no actual proof to support their use. The total success rate was 68% with 12 patients undergoing permanent implantation; 10 sufferers were in a place to void usually and two sufferers still wanted to catheterize. It is usually nicely tolerated and secure and supplies a helpful therapeutic choice to restore voiding in these sufferers. There is a sustained detrusor contraction of >50 cm H2O with failure of the bladder neck to open. Marion (1933) originally described it in a male affected person, but its presence in women was discovered by Diokno et al. Another is that a continuing excessive tonus within the easy muscle of the posterior urethra causes rigidity of the bladder neck. A theory that an elevated number of -adrenergic receptors resulting in nonrelaxation during voiding additionally has been suggested. They showed that sufferers with dysfunctional voiding have greater imply most move fee (12 versus 7 mL/s, P = 0. The number of those who elect observation and have progressive signs, decompensation, or even go on to obtain remedy is unknown. This could be done both unilaterally or bilaterally, but the main concern of bladder neck incision is the event of postoperative stress incontinence. The concept of bladder neck incision initially was described by Turner-Warwick et al. A 76% success price at imply follow-up of fifty five months was obtained; one patient (3%) developed incontinence. Twenty-five sufferers have been out there for follow-up at five years, and there was important enchancment in each subjective and goal voiding capabilities. Voiding dysfunction attributable to pelvic prolapse could be treated by a pessary or surgical restore.
Raloxifene 60mg cheap
Sutured Rectopexy Cutait (1959) first described fixation of the rectum with suture as a element of remedy for rectal prolapse. Whether synthetic materials ought to be used within the setting of bowel resection is controversial, as a end result of the chance of an infection could additionally be elevated. Excellent outcomes have been obtained in a selection of collection by which the lateral rectal stalks had been sutured to the presacral fascia, with recurrence charges starting from 3% to 9%. A downside of this method, nevertheless, is the development of new-onset constipation in 15% of patients or worsening constipation in sufferers (50%) with existing constipative signs. Questions stay regarding the added benefit of sutured rectal fixation after rectal mobilization. One randomized trial has examined the good factor about rectopexy versus no rectopexy after rectal mobilization within the treatment of prolapse (Karas et al. Ripstein Procedure In 1963, Ripstein and Lanter described an anterior rectopexy involving using prosthetic material. After mobilization of the rectum, the rectopexy is performed by inserting a long strip of mesh (5 � 20 cm) around the rectum and suturing the free ends of the mesh to the presacral fascia with nonabsorbable sutures. The rectum is pulled straight out of the pelvis while the sutures are being positioned. The mesh is wrapped loosely enough to allow a thumb or two fingers between the rectum and the sacrum. Alternatively, some surgeons safe the mesh to the presacral fascia on the mid portion of the mesh and wrap every free end across the rectum, securing the ends to the antimesenteric border of the rectum. This modification makes an attempt to decrease the rate of impaction or obstruction seen when the mesh fully encircles the rectum. Indeed, Ripstein now uses the posterior rectal sling rather than an anterior sling to lower problems with constipation. The Ripstein procedure has been praised for its low prolapse recurrence price and criticized for postoperative obstructive complications. Gordon and Hoexter (1978) polled the members of the American Society of Colon and Rectal Surgeons, obtaining data on 1111 Ripstein procedures. Postoperative constipation should be interpreted rigorously as many sufferers who endure prolapse surgery expertise constipation preoperatively. However, 35% of sufferers were dissatisfied after the Ripstein process, based on a private interview using a standard questionnaire, regardless of anatomic correction of the prolapse. Due to these outcomes, we have a tendency not to carry out Ripstein procedures in sufferers with preoperative obstructive symptoms or vital bowel dysfunction. This variation of mesh rectopexy entails anterior mobilization of the rectum with mesh fixation of the anterior rectal wall and fixation of mesh to the sacrum. Although there have been no randomized trials evaluating ventral with posterior rectopexy, a number of systematic evaluations have famous an appropriate recurrence price (3. Despite these improvements in end result, ventral rectopexy has been associated with an increased total complication fee (up to 47% in some series), with issues that included mesh erosion into vagina or rectum and pelvic sepsis from mesh infection. The unique idea was primarily based on the concept of suspending the left colon from the splenic flexure to cut back prolapse recurrence. Subsequent research have demonstrated that recurrence charges are comparable with and without sigmoid resection, as low as 2% to 5% in some collection. We carry out rectopexy with resection by mobilizing the sigmoid colon and dividing the mesentery. We favor to resect the sigmoid colon and subsequent perform the anastomosis either as hand-sewn or with the circular stapler. Patients with preoperative constipation reported decrease constipation charges after resection rectopexy versus rectopexy alone. Patients with preoperative fecal incontinence might report an improvement of their symptoms after resection rectopexy, however decision of fecal incontinence is far less widespread after sigmoid resection. Minimally Invasive ApproachesLaparoscopy and Robotics the issue in choosing between an belly method and a perineal method for the therapy of rectal prolapse is choosing between a lower recurrence fee (abdominal approach) and a lower surgical morbidity (perineal approach), as many patients with rectal prolapse are aged and have important comorbidity. A laparoscopic method is conceptually engaging as it combines the advantages of each approaches. Since laparoscopic rectopexy was first carried out in 1992 by Berman, many research have assessed and supported its feasibility and effectiveness in treating rectal prolapse. There have been two prospective studies and a number of other observational research since this time which have shown persistently reduced postoperative ache, shortened hospital size of stay, and earlier return of bowel perform in sufferers present process a laparoscopic strategy in contrast with the open method. Operating time was significantly longer for laparoscopic compared with open circumstances (153 versus 102 min), but the length of hospital stay was shorter (3.
Generic 60 mg raloxifene visa
A paravaginal defect restore is carried out, if wanted, to deal with anterior vaginal wall defects. If rectal prolapse is current, a rectopexy with or without sigmoid resection can be performed laparoscopically with or with out robotic help. Robotic Sacral Colpopexy the robotic sacral colpopexy is carried out using a way much like the laparoscopic sacral colpopexy. The da Vinci Surgical System has three elements: the affected person cart (operative robot), surgeon console, and the imaginative and prescient cart. The robotic strategy to sacral colpopexy differs from the laparoscopic strategy on a couple of parameters: trocar areas, docking the robotic affected person cart, and use of intracorporeal knot tying. A 12 mm umbilical trocar is used for the laparoscope, and an eight mm assistant trocar is positioned 9 cm lateral to the right-sided robotic trocar. After first affixing the camera arm, the other robotic arms are connected to the robotic trocars with care taken to place arms to decrease risk of robotic arm collisions. A 30� angle between the instruments arms and camera is sweet, however a 45� angle is usually better. If a hysterectomy is being performed, the Tenaculum Forceps could be placed in arm 3, somewhat than the Prograsp; however, this is only essential for big uteri with fibroids. Once the preliminary dissection for the sacral colpopexy is completed, we usually use a SutureCut needle driver in arm 1, needle driver in arm 2 and Prograsp in arm 3 to suture robotically with 8-in monofilament 2-0 or 0 polypropylene and polydioxanone, as described above in our dialogue of laparoscopic sacral colpopexy. Consequently, a surgeon ought to be comfy with the options of the particular robotic system before its use. Robotic arms are optimally 30� to 45� from each other with the fourth arm (arm 3) often positioned almost parallel to the ground. Clinical Results: Subjective and Objective Cure In the current replace of the Cochrane review of surgical administration of pelvic organ prolapse, Maher et al. The particulars of these trials and their findings are discussed below and summarized in Table 21. Only a couple of well-designed comparative studies exist, and many have various goal and subjective outcomes. One single-center, blinded, randomized trial from our institution randomized women with post-hysterectomy stage 2 to 4 vaginal apex prolapse to both laparoscopic or robotic sacrocolpopexy (Paraiso et al. The major outcome was whole operative time from incision to closure, however secondary outcomes included postoperative pain, functional activity, bowel and bladder symptoms, quality-of-life, anatomic vaginal assist, and cost from a health care perspective. Total operative time was considerably longer in the robotic group (227 � 47 versus 162 � forty seven min; P < zero. In addition, sacral colpopexy suture tying was longer for the robotic group (98 � 22 versus sixty eight � sixteen min; P < zero. We believe that elevated ache within the robotic group was caused by muscular ache associated with manipulation and fascial closure of the best paracolic gutter accessory port. Secondary outcomes were intraoperative blood loss, mean drop in hemoglobin, length of postoperative hospitalization, operating time, postoperative pain evaluation, return to day by day actions, high quality of life, new onset of urinary incontinence, and reoperation charges. At 1 yr, level C met equivalence criteria for the stomach and laparoscopic groups (6. Secondary outcomes have been patient satisfaction, high quality of life outcomes, complications, and reoperations. Although imply affected person satisfaction scores (0-100) had been significantly greater in the laparoscopic sacral colpopexy group (87 � 21 versus 79 � 20; P = 0. Four hundred patients in the cohort underwent open sacral colpopexy, 231 underwent laparoscopic, and 218 had robotic-assisted laparoscopic sacral colpopexy. Laparoscopic and robotic cases were analyzed as minimally invasive sacral colpopexy. Anatomic failures had been larger within the open group compared with the minimally invasive group (24. Compared with ladies who underwent minimally invasive sacral colpopexy, women undergoing open sacral colpopexy had a better operative blood loss (188 versus 122 mL; P < 0.
Ormenis nobilis (Roman Chamomile). Raloxifene.
- Dosing considerations for Roman Chamomile.
- Indigestion, nausea, vomiting, painful periods, sore throat, sinusitis, eczema, wounds, sore nipples and gums, liver and gallbladder problems, frostbite, diaper rash, hemorrhoids, and other conditions.
- Are there safety concerns?
- How does Roman Chamomile work?
- What is Roman Chamomile?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96734
Discount raloxifene 60 mg overnight delivery
The specialists in deciding whether or not a suggestion is applicable to a given affected person is the patient and providers not the researchers and academicians who critically appraise analysis findings. The differing experience wanted to put together systematic evaluations regarding the evidentiary base of a suggestion and to establish implementation potential highlights the inappropriateness of researchers telling practitioners and sufferers what pointers to use. There is an attempt to promote candidness and readability instead of secrecy and obscurity. Medical educators and clinicians want scientific bases for determining "greatest apply" approaches along with the analysis and statistical tools to learn how to assess the outcomes of research to improve patient care. This strategy integrates individual medical experience with greatest obtainable proof (relevant studies found from a scientific search of the well being care literature). Practicing evidence-based medicine implies not solely clinical experience (proficiency and judgment acquired through experience), but experience in retrieving, deciphering, and applying the results of scientific studies, and in speaking the risks and benefits of various courses of action to sufferers. First, each time potential, apply must be grounded on prior findings that show empirically that certain actions carried out with a specific kind of patient are likely to produce predictable, beneficial, and effective results. Efforts are made to put together complete, rigorous evaluations of all research associated to questions of effectiveness, prevention, screening (risk and prognosis), description and evaluation, harm, and self-development. He/she will need to (1) know how to learn and critique analysis articles and (2) assess the diploma to which an intervention has been empirically examined and located promising. To entry, analyze, and apply analysis findings in diabetic studies, practitioners might want to understand why, by whom, and how analysis research are conducted. Therefore, medical faculty and continuing medical training will want to educate and reinforce the research of analysis design-the overall framework for accumulating data as soon as the issue has been formulated. In addition, these establishments might need to teach how to learn and interpret the data and what they mean. The primary goal of this educational strategy shall be to integrate individual scientific expertise with critical analysis of evidence discovered from a systematic literature search to remedy an issue. Understanding what type of examine has been performed is a prerequisite to considerate studying of analysis. What is now known is that physicians, underneath the affect of pharmaceutical promoting and promotions, are rather more impressionable than was initially believed. Lots of zeroes might look spectacular in analysis findings yet they nonetheless amount to zero. Unfortunately, most physicians lack expertise in evaluating studies for bias and relevancy. This may find yourself in harmful penalties to sufferers and is one of the reasons the enthusiastic use of the anti-inflammatory drug Vioxx caused hurt to so many patients. Clinicians confront voluminous evidence in regards to the medical selections they face every day. To treatment the issue, many medical groups concern medical practice tips: consultants in a area kind through the reams of medical analysis on a medical condition and pore over drug studies; they then publish summaries about what treatments work finest in order that physicians in all places can provide the most acceptable, up-to-date care to their patients. Several of the now promoted medication are costly newcomers that lack the track records of medical effectiveness and safety by the older, doubtlessly displaced remedies. At the end of the day, medicine, like artwork, is a artistic course of, and really a lot a team effort. Excellent well being care practice ought to be impressed by love and guided by science; both are essential. If a professional practices scientifically with out compassion, he/she turns into a robotic. Researchers and Peer Review Peer review is the primary apparatus that analysis journals use to assess the standard of the various manuscripts competing for the few places available for publication. Journal editors solicit evaluations of submitted manuscripts from outside experts who remain nameless to the authors by the method. The results of a evaluation can consecrate or doom the progress of a particular course of analysis. Negative outcomes could not all the time be reported and are also much less more doubtless to be published in prestigious journals. Despite over 300 years of use, the pursuit of excellence in analysis has not been accompanied by a parallel pursuit within the analysis of that excellence.
Purchase raloxifene without a prescription
This mannequin has important implications for the relationship between the pregnant woman and the obstetrician. The maternal-rights-based reductionist model has a radical implication that its advocates ignore. There are solely sick individuals (aegrotrus within the Latin texts that precede Gregory and Percival in the historical past of Western medical ethics) or shoppers who contract with providers. In the skilled duty model of obstetric ethics, when the fetus is a affected person, directive counseling for fetal benefit is ethically justified. In clinical apply, directive counseling for fetal profit includes a number of of the next: recommending towards termination of pregnancy; recommending towards nonaggressive management; or recommending aggressive management. Aggressive obstetric administration consists of interventions corresponding to fetal surveillance, tocolysis, cesarean supply, or supply in a tertiary-care heart when indicated. Directive counseling for fetal profit, nonetheless, should all the time keep in mind the presence and severity of fetal anomalies, excessive prematurity, and obligations to the pregnant woman. As a rule, the more extreme the fetal anomaly the much less directive counseling ought to be for fetal profit. In specific, this is the case for what we term just-viable fetuses,1 those with a gestational age of 24�26 weeks, for which there are important charges of survival however excessive rates of mortality and morbidity. Thus, it would appear that there are substantial beneficence-based obligations to just-viable fetuses to provide aggressive obstetric administration. Directive counseling for fetal profit must at all times occur within the context of balancing beneficence-based obligations to the fetus against beneficence-based and autonomy-based obligations to the pregnant woman1,14 Table 1-1). Any such balancing should acknowledge that a pregnant girl is obligated solely to take reasonable dangers of medical interventions which are reliably anticipated to benefit the viable fetus or child later. Such conflict is greatest managed preventively by way of knowledgeable consent as an ongoing dialogue throughout the pregnancy, augmented as needed by negotiation and respectful persuasion. If she does confer such standing in a settled means, at that time beneficence-based obligations to her fetus come into existence and directive counseling for fetal benefit becomes applicable for these fetuses. Just as for viable fetuses, such counseling must always additionally bear in mind the presence and severity of fetal anomalies, excessive prematurity, and obligations owed to the pregnant girl. For pregnancies during which the girl is unsure about whether to confer such status, the authors suggest that the fetus be provisionally considered a patient. This also justifies directive counseling about diagnostic surveillance, for instance, ultrasound examination to detect anomalies. Competing well-founded beneficence-based medical judgments regarding how to steadiness the fetal advantage of preventing hurt of cesarean supply generate these controversies, that are discussed elsewhere in this volume. This strategy empowers the girl to emphasize her own perspective in balancing maternal and fetal advantages and risks. Although cesarean supply is supported in beneficence-based scientific judgment, trial of labor is more substantively supported. Therefore, the skilled accountability mannequin helps offering and recommending trial of labor. The skilled duty model of obstetric ethics offers dependable, clinically applicable steering for the management of these challenges. This method is designed to prevent conflict between the obstetrician and the pregnant woman about intrapartum management. We have deployed this model to tackle when to supply and advocate cesarean delivery. We consider that the medical application of the professional accountability model of obstetric ethics will strengthen the obstetrician�patient relationship and, subsequently, enhance the quality of take care of pregnant ladies with diabetes. The professional duty mannequin of obstetric ethics: avoiding the perils of clashing rights. Clinical guides to preventing ethical conflicts between pregnant ladies and their physicians. The discourses of European practitioners within the tradition of the Hippocratic texts. Hippocratic beliefs, medical ethics, and the apply of medication in the early center ages: the legacy of the Hippocratic Oath. John Gregory and the Invention of Professional Medical Ethics and the Profession of Medicine.
Cheap 60 mg raloxifene otc
Diagnosis and remedy of gestational diabetes according to amniotic fluid insulin ranges. Industrialized countries are currently experiencing an epidemic of weight problems and a rising incidence of diabetes. Increased glucose uptake by skeletal muscle is partly attributable to increased muscle perfusion during exercise. Exercise results in beneficial alterations in physique composition and biochemical, physiological, and morphological modifications in skeletal muscles. Exercise in an overweight girl results in weight loss and the percentage of type 1 muscle fibers increases, resulting in elevated muscle oxidative capability. In addition to these factors, train may relieve stress, scale back anxiousness, and despair, and improve self-confidence and, in doing so, limit "emotional consuming" that contributes to weight gain and insulin resistance. Increased physical exercise often leads to improvements in self-image and different components that, in turn, assist wholesome life type. After an exercise session, glucose tolerance is improved for variable periods depending on the mass of the muscle activated, length, intensity, and insulin response. Essential to this process that leads to improved insulin sensitivity and glucose uptake is the activation of particularly massive muscular tissues such because the quadriceps. There has lengthy been concern that exercise throughout pregnancy might enhance the risk of preterm supply, fetal development restriction, or fetal distress because of a decrease within the uterine blood circulate throughout train that would have an result on the fetus and lead to an abnormal fetal coronary heart price and different physiologic responses that might be harmful to the fetus and even lead to fetal demise. In the nonpregnant lady, goal coronary heart rates have been regularly used to prescribe train. In regard to prescribing train depth, however, it should be acknowledged that in pregnancy maximal maternal heart fee reserve decreases and resting coronary heart fee increases. There are few research in being pregnant combining diet and train; nevertheless, evidence is emerging that both train and weight restrictions are protected interventions in obese and overweight pregnant ladies. A triad of pregravid weight problems, excessive gestational weight acquire, and diabetes in pregnancy are sometimes discovered in combination. Each of these elements independently increases the danger of fetal overgrowth and, in turn, childhood weight problems. In our expertise, minimally to no weight gain in overweight girls has no deleterious influence on the fetus and is helpful to the mom in regard to her long-term 3. Hypoglycemia may end result when a pregnant girl exercises and her glucose level is depressed secondary to fasting or medicine. The danger of hypoglycemia is greatest in early being pregnant, previous to the fall in insulin-mediated glucose disposal that occurs over the course of the second and third trimesters. Over the previous 30 years, our laboratory has performed studies examining the influence of being pregnant on maternal and fetal responses to exercise, on the regulation of glucose homeostasis by glucagon, insulin, and catecholamines and different. After 45 minutes, glucose concentration declined additional, suggesting that at this point the potential threat of hypoglycemia with moderate-intensity continuous train might rise. Preexisting and pregnancyinduced low-back ache and joint ache are also widespread issues. Pregnant women with these limitations could also be extra tolerant of nonweight-bearing train. Many of the person trials that have investigated the influence of bodily exercise on gestational weight gain have been limited by their small dimension and poor participant compliance. Recognition of these limitations have prompted a 2011 meta-analysis of 12 bodily activity intervention trials that collectively enrolled over a thousand girls. The evaluation uncovered a modest however statistically vital reduction in gestational weight achieve amongst those uncovered to varied physical activity interventions. That meta-analysis included five potential cohort, two retrospective case-control, and two cross-sectional studies. This means that an exercise program, although beneficial to all is more practical in preventing gestational diabetes in chubby or obese ladies, somewhat than in regular weight women. The other five trials had been initiated earlier in being pregnant however the majority if not all the various interventions had been carried out within the second and third trimesters, and the ability of the trials was limited by their small dimension, starting from a total of forty one to 142 individuals. Only one of the research included in this 2013 meta-analysis restricted enrollment to overweight pregnant women. The intervention concerned twice weekly 60-minute aerobic and energy train sessions that began round 15 weeks of gestation. That threat is essentially due to decreased hypoglycemic consciousness and counter-regulatory adaptations which could be altered by pregnancy-related augmentation of catecholamine and glucagon responses.