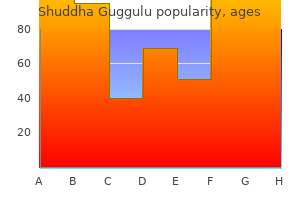
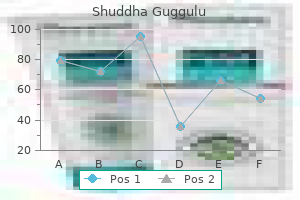
Shuddha Guggulu dosages: 60 caps
Shuddha Guggulu packs: 1 bottles, 2 bottles, 3 bottles, 4 bottles, 5 bottles, 6 bottles, 7 bottles, 8 bottles, 9 bottles, 10 bottles
Purchase shuddha guggulu 60caps with amex
The proximal fibulae are hypoplastic, and the distal fibulae are wide with irregular contours. Minor facial dysmorphism in Laurin-Sandrow syndrome: hypoplastic alae nasi, depressed nasal tip, and quick columella. Preaxial triphalangeal polysyndactyly of the digits and toes, predominantly in the lower limb. Rarely associated with visceral anomalies, similar to cryptorchidism, congenital coronary heart disease, and Hirschsprung illness. The radii and ulnae are often unremarkable, but they could be hypoplastic; ulnar duplication could happen. Malformation of the hand is usually triphalangeal thumb, however preaxial polysyndactyly and mirror-image hand might occur. The mutations are liable for the tibial hypoplasia with polydactyly phenolype whereas the duplications for Laurin-Sandrow syndrome. A lethal case of Werner sort with encephalocele, microphthalmia, and urogenital anomalies has also been reported. The proper foot (left image) has seven toes, whereas the left foot (right image) has eight toes. There is fibular duplication bilaterally: two bones are almost equivalent to each other in shape on the best, while the midshaft of the medial bone is missing on the left. The postaxial three fingers show full cutaneous syndactyly ("mitten hand"), and the preaxial first fingers are triphalangeal. The left hand reveals preaxial triphalangeal polydactyly and the best thumb is triphalangeal as well. The distal ulnae are broader than the distal radii, implying partial duplication of the ulnae. Micrognathia with cleft palate; other variable facial abnormalities, together with crumpled ear, distinguished eyes, epicanthic folds, and broad nasal root. Bowing of the forearm and leg related to a cutaneous dimple on the apex of bowing; restriction of the elbow joint. Posterior bowing of the ulnae with spur formation; the radii are posteriorly bowed or subluxed. Bowing of the fibulae and/or tibiae with spur formation; anterior bowing is widespread, however posterior bowing might happen. However, campomelic dysplasia is distinguishable from Reardon-Kozlowski kind on the overall radiological pattern and/or molecular grounds. Some cases that had been reported as kyphomelic dysplasia could be the similar dysfunction as Reardon-Kozlowski sort. Pseudodiastrophic dysplasia: A stillborn sibling of a patient with pseudodiastrophic dysplasia had severe bowing of the long bones, which resembled that of ReardonKozlowski kind (Yap et al. To date, there have been only two reports on the Reardon-Kozlowski kind (Reardon et al. Kozlowski K, Bacha L, Brachimi L, Massen R (1993) Mesomelic dysplasia of the higher extremities related to other abnormalities: a new syndrome Probably autosomal recessive; affected siblings born to a consanguineous couple have been reported. Underossification of the spine and pelvis might be because of the early gestational age. The ulna and radius are very brief, and the proximal ulna and radius show sharp angulation with bone spur. There are gentle platyspondyly and Perthes-like flattening of the proximal femoral epiphyses. Marked shortening and deformity of the lower legs with bony prominence and cutaneous dimple. Mild to average shortening of the forearms; restricted mobility of the elbow joint. May be associated with different musculoskeletal abnormalities: hip dislocation; malalignment of the knee joint with patellar dislocation; variable anomalies of the toes and digits (oligosyndactyly and polydactyly). The instances with abnormal patterning of digits are sometimes termed Nievergelt-like syndrome. Shortening and triangular or rhomboid shape of the tibiae with epiphyseal brackets; less marked shortness and widening of the fibulae, radii, and ulnae. Radioulnar synostosis; dislocation or subluxation of the radial head and barely the proximal ulna.
Diseases
- Costocoracoid ligament congenitally short
- Hereditary carnitine deficiency myopathy
- Odynophobia
- Macrosomia microphthalmia cleft palate
- Radioulnar synostosis mental retardation hypotonia
- Neurocutaneous melanosis
- Reactive attachment disorder of infancy
- Cleft lip palate abnormal thumbs microcephaly
Buy shuddha guggulu from india
Invasive angiography is of limited diagnostic value due to the regularly small quantity of the fistulas. The clinical presentation of aortoenteric and aortopulmonary fistulas is highly variable and includes acute and persistent, mild or extreme hematochezia or hematemesis. Other attainable manifestations are again pain or extended, often subacute indicators of an infection (prosthetic infection). Aortopulmonary fistulas are distinguished by various levels of hematemesis and hemoptysis. Massive hemoptysis at a rate of 300 to 400 mL of blood/24 hours is strongly suspicious for an aortopulmonary fistula. Apart from earlier surgical procedure, malignancies are a particularly frequent explanation for aortopulmonary fistulas, in which case the signs of 98 Downloaded by: Tulane University. Postoperative histology after vena cava substitute confirmed a main angiosarcoma of the inferior vena cava. This discovering is suggestive of an aortoduodenal fistula associated with an aortic aneurysm. In some instances hemoptysis could even be falsely attributed to a fistula quite than an underlying tumor. All aortic fistulas current with episodes of decreased hemoglobin ranges and low blood pressure. Immediate remedy, which is normally surgical and rarely interventional, is necessary as a result of the very high mortality in untreated instances. The differential prognosis of aortoenteric fistula contains simple aortitis, prosthetic infection, mycotic aneurysm, retroperitoneal abscess, and retroperitoneal fibrosis. The differential diagnosis of aortopulmonary fistulas contains main and secondary lung malignancies and granulomatous inflammations, especially tuberculosis. Aortoenteric and aortopulmonary fistulas are a rare and tough analysis on imaging. Typical medical signs outcome from the arteriovenous shunt and its typically excessive circulate volume and current with right heart failure and possible decrease extremity edema. Besides surgical ligation, the implantation of stent grafts has become a first-line remedy option. Aortocaval fistula is a rare complication that outcomes predominantly from the confined perforation of an aortic aneurysm. This results in retrograde flow in the vertebral artery on the affected facet, which diverts blood away from the mind to the ipsilateral arm. Other cases are attributable to postoperative adjustments, postirradiation adjustments, trauma, arteritis, or a thoracic outlet syndrome. Because most sufferers are asymptomatic, the true prevalence of the disease is unknown however is believed to be in the range 0. The more frequent cause is the contained rupture of an aortic aneurysm into the inferior vena cava. Large Vessels Coexisting coronary steal syndrome has also been described as a variant; it arises from the same pathology but causes retrograde circulate in an ipsilateral inside mammary artery bypass graft. Conventional angiography, whereas still the diagnostic gold commonplace, has been almost utterly discontinued in routine settings because of its inherent complications. It should still be used within the setting of interventional remedy, which has turn into the established medical standard. Most sufferers are asymptomatic, but medical examination could reveal a typical blood stress discrepancy between the arms. Classic symptoms contain the posterior cerebral circulation and consist of dizziness, ataxia, nystagmus, syncopal assaults, or visual disturbances. An inadequate collateral provide could result in atypical signs such as arm and hand weakness and coldness and paresthesias within the affected limb. In patients with a coexisting coronary steal syndrome, signs of cardiac ischemia or angina pectoris could be the solely discovering. Symptoms may be evoked by stress maneuvers such as turning the top to the opposite facet or elevation of the arm. The primary differential prognosis is stroke as a potential reason for neurologic symptoms. Other neurologic illnesses corresponding to cerebellar tumors or a quantity of sclerosis might have related manifestations.
Generic shuddha guggulu 60 caps on-line
This situation rarely inter eres with respiration however o ten is corrected surgically or cosmetic causes. The ribs are common sites o metastatic lesions, which may be characterized and visualized on the image as ollows: steol tic- damaging lesions with irregular margins � steoblastic- proli erative bony lesions o elevated density � moth-eaten appear� Com bination osteol tic an osteoblastic- ance o bone ensuing rom the combo o destructive and blastic lesions steom elitis: this localized or generalized in ection o bone and marrow could be related to postoperative problems o open heart surgery, which requires the sternum to be break up. Ro utine andSpe cialPro je ctio ns Protocols and positioning routines differ amongst acilities, relying on administrative structures, liabilities, and different actors. Certain routine and special projections or the sternum, sternoclavicular joints, and ribs are demonstrated and described on the ollowing pages as suggested standard routine and special departmental routines or procedures. Per orm research erect when potential Routine radiographic sternum views, computed tomography Disruption o bony cortex o the rib; linear lucency by way of the rib Disruption o bony cortex o the sternum; linear lucency or a displaced sternal phase Anterior protrusion o decrease sternum Depressed sternum Depends on lesion type: � Destructive: irregular margins and decreased density � Osteoblastic lesions: increased density � Combination- moth-eaten appearance Erosion o bony margins None None Congenital anomalies Pectus carinatum (pigeon breast) Pectus excavatum (unnel chest) Metastases Routine chest and potential lateral sternum Routine chest and attainable lateral sternum Routine radiographic views, nuclear medication bone scan None None None or enhance (+) or lower (-), relying on type o lesion and stage o pathology Osteomyelitis Routine sternum views, nuclear medication bone scan None *Dependent on stage or severity o illness or condition. Positio n: � Correct affected person rotation is demonstrated by visualizing sternum alongside vertebral column with no superimposition by vertebrae. Exp o su re: � Optimal contrast and density (brightness) reveal outline o sternum through overlying ribs, lung, and coronary heart. Re sp ira tio n Orthostatic (shallow breathing) method could be per ormed i patient can cooperate. Orthostatic breathing method requires a minimal o a 3-second publicity time and a low mA to produce blurring o overlying vascular structures. A transportable grid can be required and must be placed crosswise on the stretcher or tabletop to stop grid cuto. Po sitio n: Correct patient place with no rotation demonstrates the ollowing: � No superimposition o humeri, shoulders, or so t tissue on sternum. Exp o su re: � Optimal contrast and density (brightness) to visualize the complete sternum. Po sitio n: � o rotation o affected person, as demonstrated by equal distance o sternoclavicular joints rom vertebral column on either side. Exp o su re: � Optimal contrast and density (brightness) to visualize the manubrium and medial portion o the clavicles via superimposing ribs and lungs. Po sitio n: � Correct affected person rotation demonstrates the draw back sternoclavicular joint visualized with no superimposition o the vertebral column or manubrium. Exp o su re: � Optimal contrast and density (brightness) to visualize the sternoclavicular joints through overlying ribs and lungs. Exp o su re: � Optimal distinction and density (brightness) to visualize ribs via the lungs and coronary heart shadow or via the dense stomach organs i under the diaphragm. Exp o su re: � Optimal contrast and density (brightness) to visualize ribs through the lungs and coronary heart. Re sp ira tio n Suspend respiration on inspiration or ribs above the diaphragm and on e piration or ribs beneath the diaphragm. Pa rt sitio n Po � Rotate affected person into 45� posterior or anterior indirect, with affecte si e closest to on posterior indirect and affecte si e awa from on anterior indirect. Evaluatio nCrite ria bove- iaphragm ribs: Ribs 1 by way of 9 must be included and seen above the diaphragm. Po sitio n: � An accurate 45� oblique place should reveal the axillary ribs in pro le with the backbone shi ted away rom the area o interest. As a starting critique exercise, place a verify in every category that demonstrates a repeatable error or that radiograph. Student workbooks provide extra space or writing comments and complete critique solutions or every o these radiographs. The anatomy o the cranium could be very complicated, and specif c consideration to detail is required o the technologist. Anatomy and positioning or the cranial and acial bones are described in this chapter. These cranial bones are used in an grownup to orm a protecting enclosure or the brain. Each o these cranial bones is demonstrated and described individually in the pages that ollow. This bone contributes to the ormation o the orehead and the superior part o every orbit. It consists o two main components: the squam us or v rtical p rti n, which orms the orehead, and the rbital or h riz ntal p rti n, which orms the superior half o the orbit. Below the orbital plates lie acial bones, and above the orbital plates is the anterior half o the oor o the brain case. The lateral walls o the skull and part o the roo are ormed by the two parietal bones.
Order shuddha guggulu 60caps without a prescription
Pectoralis minor syndrome: compression of the neurovascular bundle by the pectoralis minor tendon attachment to the coracoid process. The chest radiograph can set up the presence of cervical ribs and in addition reveal the purpose for an atypical compression syndrome as a result of exostoses or old fractures. A pure thoracic inlet syndrome with thrombosis of the subclavian vein and potential involvement of the tributary axillary and brachial veins virtually invariably outcomes from costoclavicular compression, while a pure thoracic outlet syndrome is because of compression by a cervical rib. All other forms often trigger blended neurologic and vascular symptoms with pain, dysesthesia, and muscle weak point or even paralysis as the neurologic element. In sufferers with thoracic outlet syndrome, elevation of the arm results in ipsilateral chilly sensation, weakness, and loss of the peripheral radial artery pulse. Venous compression results in venous congestion issues marked by pain, heavy sensation, and potential venous thrombosis. The differential diagnosis is advanced and includes focal neurologic causes corresponding to radiculopathy or plexopathy, ulnar groove syndrome, and carpal tunnel syndrome in addition to systemic neurologic ailments similar to multiple sclerosis. Combinations may be encountered, similar to a double crush syndrome in which thoracic outlet or inlet syndrome is combined with carpal tunnel syndrome. A thoracic outlet or inlet syndrome because of neurovascular compression on the superior thoracic aperture can have various causes. Diagnosis depends on chest radiographs and on invasive angiography or venography with provocative hyperabduction, relying on whether or not arterial or venous symptoms are present. Venous anatomy is variable, relying on the persistence or regression of those giant embryonic veins. Development of the veins proceeds as follows: the vitelline veins give rise to the portal venous system and the posthepatic segment of the inferior vena cava. The initially paired umbilical veins type early connections with hepatic sinusoids. While the proper umbilical vein regresses at an early stage, the ductus venosus develops to type a connection between the left umbilical vein and proper heart. At birth this channel is obliterated and varieties the hepatic spherical ligament and ligamentum venosum. The paired anterior cardinal veins type the systemic veins for the upper half of the body. In addition to the cardinal veins, the paired subcardinal veins are fashioned between the fifth and 3. The left brachiocephalic vein passes behind the sternum and is significantly longer than the proper brachiocephalic vein. The azygos vein runs a substantial right paravertebral course earlier than opening into the superior vena cava, draining the posterior parts of the chest and abdomen. Its counterpart on the left aspect is the hemiazygos vein, which drains into the azygos vein at a variable intrathoracic degree. The venous anatomy of the stomach is fashioned by the bilateral iliac veins; each drain into the inferior vena cava, which ascends just to the right of the vertebral column. Internal jugular vein Subclavian vein Right brachiocephalic vein Superior vena cava Supreme intercostal vein Subclavian vein Left brachiocephalic vein Right superior intercostal vein Accessory hemiazygos vein Azygos vein Hemiazygos vein Persistent Left Superior Vena Cava Brief definition. Embryologically, a persistent left superior vena cava outcomes from persistence of the left anterior cardinal vein. The left brachiocephalic vein usually forms a communication between the left and proper superior vena cava. This increases to as much as 5% when different congenital cardiac anomalies are current. With duplication of the inferior vena cava, this will likely sometimes be misinterpreted as a protracted iliac vein with a high iliac bifurcation, for instance. Sectional imaging aids prognosis by demonstrating a large, left retroperitoneal vein that terminates on the left renal vein. These variants are usually asymptomatic; they turn out to be vital when issues come up. There are reviews of pulmonary embolism occurring despite the placement of a vena cava filter in sufferers with a duplicated inferior vena cava, as thrombi are still able to escape through the left-sided inferior vena cava. The right subcardinal vein ultimately forms the renal segment of the inferior vena cava, while the left subcardinal vein largely regresses. The right subcardinal vein types the rest of the inferior vena cava, while the anastomosis between the subcardinal veins forms the left widespread iliac vein. Note Retroperitoneal lymphadenopathy is an important scientific differential diagnosis for an inferior vena cava variant.
Reynoutria japonica (Hu Zhang). Shuddha Guggulu.
- Are there any interactions with medications?
- Are there safety concerns?
- Dosing considerations for Hu Zhang.
- What is Hu Zhang?
- Constipation, menstrual problems, hot flashes, heart disease, high cholesterol, cancer, skin burns, liver disease, gout, and gallstones.
- How does Hu Zhang work?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=97057
Purchase shuddha guggulu 60caps on-line
Two kinds of distortion have been identi ed: measurement distortion (magni cation) and form distortion. Nevertheless, distortion could be minimized and managed if some fundamental ideas are used as a guide. The eld measurement of the x-ray beam is limited by a collimator that consists of adjustable lead attenuators or shutters. The collimator and shutters take up the x-rays on the periphery, controlling the scale of the x-ray beam. Greater magni cation is demonstrated at the periphery (A and B) than at the level of the central ray (C). It is essential for technologists to control intently and decrease distortion as much as possible. Co n tro llin g cto rs Fa Following are fou primary controlling elements of distortion: 1. Distortion increases as the angle of divergence increases from the middle of the x-ray beam to the outer edges. For this purpose, right centering or correct central ray alignment and placement is necessary in minimizing image distortion. Although digital imaging differs from lm-screen imaging in phrases of the method of picture acquisition, elements which will affect x-ray production, attenuation, and geometry of the x-ray beam still apply. In diagnostic imaging, each pixel represents the smallest unit within the image; columns and rows of pixels make up the matrix. The sequence of squares on the sheet could be in contrast with the matrix, and each individual sq. can be compared with a pixel. Digital processing involves the system tic pplic tio of highly com plex m them tic l fo m ul s referred to as algorithms. Numerous mathematical manipulations are performed on image data to improve picture appearance and to optimize quality. Algorithms are utilized by the pc to each information set obtained earlier than the technologist sees the image. The exposure latitude for a digital imaging system is de ned as the appropriate stage of publicity that produces the desired image quality for the division. Note that the rise from 1 to eight mAs still produces a diagnostic image of the elbow. It have to be remembered, nonetheless, that the kV and mAs used for the publicity affect affected person dose. A bene t of using a higher kV is that patient dose is lowered as compared with lower kV ranges. Compared with lm-screen imaging, changes in kV can have much less of a direct impact on nal digital picture distinction because the resultant contrast can additionally be a function of the digital processing. Co n tro llin g cto rs Fa Digital imaging techniques are designed to show electronically the optimal picture brightness beneath a variety of publicity components. Brightness is controlled by the processing software program by way of the application of predetermined digital processing algorithms. Because pc theory relies on the binary system, a 14-bit system, for instance, is represented as 2 14; the 14-bit-deep pixel may represent any certainly one of 16,384 potential shades of grey, from black to white. A common radiography acquisition matrix may be 3000 � 3000 pixels- greater than 9 million pixels (9 megapixels)- a 17 � 17-inch (43 � in 43-cm) image. This is accomplished by the proper use of grids, by shut collimation, and by choice of the optimal kV Grid cut-off occurring with digital picture receptors will end in. The change in publicity indicator is as a end result of of the decrease in amount of exit radiation hanging the receptor. Contrast decision refers to the flexibility of an imaging system to distinguish between comparable tissues. Co n tro llin g cto rs Fa Digital imaging techniques are designed to display electronically optimum picture contrast under a broad range of publicity factors. Radiographic contrast is affected by the digital processing laptop by way of the appliance of predetermined algorithms, in distinction to lm-screen imaging, in which kV is the controlling factor for picture contrast. The capability of the picture processing software program to show a desired image contrast supplies the radiographer with a potential alternative to reduce entrance skin publicity to the patient via the use of higher kV ranges.
60caps shuddha guggulu
Nevertheless, given the problems related to postsplenectomy syndrome, conservative remedy is most well-liked over splenectomy whenever potential, especially in kids. There is a threat of underestimating refined indicators of splenic damage in patients with a trauma history. Given the risk of delayed rupture, these signs ought to immediate a suggestion for appropriate patient surveillance. At current, patient surveillance is increasingly favored as a substitute for splenectomy. Splenic artery aneurysm is a visceral artery aneurysm in the course of the splenic artery. Duplex ultrasound may detect a circulate sign but is usually restricted by overlying air within the abdomen. Symptomatic aneurysms cause upper abdominal pain, indicating a need for therapy. Rupture of a splenic artery aneurysm might trigger life-threatening hemorrhage into the omental bursa and free stomach cavity. Based on the guidelines of the German Society for Vascular Surgery, splenic artery aneurysms bigger than 2 cm are thought-about an absolute indication for treatment, as are symptomatic, progressively enlarging, and ruptured aneurysms. Open surgical therapy choices embody resection of the aneurysm with end-toend anastomosis of the proximal and distal segments or the use of vascular or prosthetic interposition grafts. Partially thrombosed splenic artery aneurysms could additionally be mistaken for pancreatic tumors. The image additionally reveals hyperdense free fluid around the liver and spleen, according to hemoperitoneum (long arrows). Note Splenic artery aneurysms bigger than 2 cm are thought-about at high danger for rupture and therefore require treatment. There are many hundreds of lymph nodes within the human body-their precise number is unknown. Trabeculae lengthen from the capsule into the inside of the lymph node, dividing it into several segments. Afferent lymphatic vessels pierce the capsule at multiple sites and convey the lymph to the marginal sinuses. From there the lymph flows previous the central lymph follicles, the place it interacts with the lymphocytes. Lymph nodes have a central hilum with an artery, vein, and efferent lymphatic vessel. All three modalities can determine the dimensions of a lymph node along a number of axes and can differentiate between cortex and hilum. The principal morphological standards for figuring out lymph node pathology are: Round or globular shape (instead of oval). While these criteria are sometimes used efficiently to identify gross malignant lymphadenopathy, to date there was little success in detecting micrometastases within lymph nodes utilizing imaging strategies. A peripheral aneurysm of the splenic artery (arrow) was detected incidentally in a 62-year-old man. At the time of publication (2018), nevertheless, these agents are now not obtainable on the market. Note All imaging modalities have low sensitivity and specificity for detecting micrometastases in lymph nodes. As properly as displaying morphological options, colour duplex ultrasound can even evaluate lymph node perfusion. Its strength lies in its capability to define even deeply seated lymph nodes without artifacts. Lymph node abscess: Bacterial infections might result in abscess formation in lymph nodes with typical associated imaging indicators (indistinct margins, faint hypodense or non-echo-free liquefaction with a hyperperfused wall and perifocal reaction). A regular lymph node with a fatty hilum (dashed arrow) is visible on the opposite facet.
Order 60 caps shuddha guggulu fast delivery
The left corpus cavernosum ([a]�[d], stars) is enlarged and has displaced the best corpus cavernosum towards the opposite side. The affected portion of the left corpus cavernosum shows heterogeneous low sign depth on T2 W images (a, b). The corresponding low signal intensities within the T1 W picture (c) support the suspicion of organized thrombosis. A discontinuity is current at a typical website within the tunica albuginea (arrows) at the junction of the center and distal thirds of the penis. The ureter proximal to the fracture website is dilated and crammed with blood ([d] open arrow). The distinction is generally depicted extra clearly on T2 W photographs, though an accompanying hematoma can mask a tear. In these circumstances the absence of hematoma enhancement after administration of distinction medium will counsel the correct prognosis. A penile fracture usually causes an audible snap at the time of harm, accompanied by sudden onset of pain and immediate lack of erection. Associated hematoma is commonly current and is mostly confined to the penis however may unfold to the scrotum, perineum, and thigh. Concomitant urethral injury may be missed, so the corpus spongiosum ought to be carefully evaluated at imaging. A traumatic fracture of the tunica albuginea is associated with a snapping sound and pain of sudden onset. The penile carcinoma (stars) is barely hypointense to the corporal bodies within the T2 W images (a, b). The carcinoma shows much less enhancement than the corporal our bodies after administration of contrast medium (c, d). The inguinal lymph nodes exhibit regular dimension and shape on each side (open arrow), indicating that inguinal lymph node metastasis has not occurred. Squamous cell carcinoma of the penis typically presents initially as a painless, focal epithelial thickening on the glans penis; there may be an related ulcer. The prognosis is good in the absence of corporal invasion or lymph node metastasis. The clinical differential diagnosis contains soft or hard chancre and condylomata acuminata. Penile carcinoma is a very rare tumor, accounting for less than 1% of all male cancers. Both penile and urethral carcinoma are hypointense to the corporal bodies on T1 W and T2 W pictures. Most penile carcinomas are squamous cell carcinomas and are manifested on the glans penis. Squamous cell carcinoma of the penis is hypointense to the corporal bodies on T1 W and T2 W photographs. Cephalad to the bottom of the prostate and lateral to the vas deferens are the paired, elongated seminal vesicles, which resemble clusters of grapes. The excretory duct of every seminal vesicle joins with the ipsilateral vas deferens to type the ejaculatory duct, which opens into the urethra on the seminal colliculus. The nerves and vessels that penetrate the prostate are sites of predilection for the extracapsular extension of prostate cancer. The peripheral zone accounts for about 70% of the prostate quantity in young men, the central zone 25%, and the transitional zone 5%. With getting older, the prostate not solely enlarges but also shows a change in relative zonal volumes as the transitional zone and, to a lesser degree, the periurethral zone turn into predominant as a outcome of benign prostatic hyperplasia (p. Each zone consists of stromal and epithelial components, the latter being greater in the peripheral zone than in the central gland. Approximately 70% of prostatic adenocarcinomas come up within the peripheral zone, 25% in the transitional zone, and 10% in the central zone. The peripheral zone generally reveals high sign intensities as a outcome of its massive glandular element whereas the central gland show decrease, heterogeneous sign intensities because of a bigger stromal part. The grapelike seminal vesicles are situated cephalad to the bottom of the prostate and appear hyperintense on T2 W pictures. The urethra appears as a triangular midline structure in the posterior third of the central gland.
Generic 60 caps shuddha guggulu visa
The interlobular bile ducts accompany the intrahepatic branches of the portal vein and hepatic vein. It occupies a small fossa on the undersurface of the liver on the junction of the best and left lobes and is fused to the liver at that location. The gallbladder extends from the porta hepatis to the anterior border of the liver. The body of the gallbladder is in touch with the duodenum and proper colic flexure. The gallbladder neck, from which the cystic duct arises, is adjacent to the porta hepatis. Note A spiral association of mucosal folds within the initial a half of the cystic duct prevents the passive drainage of bile from the gallbladder but does allow bile to enter from the widespread hepatic duct when the papilla is closed. Its quantity is variable owing to the specialized structure of the gallbladder wall. Following the branching pattern of the portal vein, they merge to type more and more larger ducts that lastly turn into the ducts of the hepatic segments. The frequent hepatic duct is shaped by the junction of the proper and left ducts, which may unite inside the liver parenchyma or just after rising from the liver. The extrahepatic duct fashioned by the union of the common hepatic duct and cystic duct is called the widespread bile duct (ductus choledochus). The papilla is a muscular valve that controls the passage of bile and pancreatic secretions into the small gut. The indirect course of the ducts via the intestinal wall helps to stop the reflux of small bowel secretions into the biliary tree. In 70% of instances the terminal segments of the common bile duct and main pancreatic duct unite at a standard junction, the ampulla of Vater. In 10% of cases the widespread bile duct and major pancreatic duct enter the duodenum at separate websites. Normal variants in the origin of the cystic artery itself could be demonstrated only by typical angiography. The portal vein occupies a far posterior position within the hepatoduodenal ligament, just behind the hepatic artery. The intrahepatic bile ducts are supplied by accompanying branches of the hepatic artery and portal vein. The regional lymph nodes are situated at the porta hepatis in the hepatoduodenal ligament. The gallbladder and bile ducts derive their autonomic nerve provide from sympathetic and parasympathetic fibers of the hepatic plexus. The scientific hallmark of cholestasis is jaundice accompanied by generalized pruritus; the itchiness is caused by the deposition of bile acids in the skin. Obstructive jaundice is characterized by beer-brown urine and pale (acholic) stools. Laboratory tests present hyperbilirubinemia and elevated alkaline phosphatase exercise. Obstructive cholestasis: brought on by a mechanical outflow obstruction within the frequent hepatic duct or frequent bile duct. Intrahepatic nonobstructive cholestasis is most commonly brought on by impaired secretion from hepatocytes and happens in the following entities, among others: All types of cirrhosis. On the other hand, jaundice attributable to a mechanical outflow obstruction 244 Downloaded by: University of Michigan. Duplication of the cystic artery, each arising from the best hepatic artery a 6 Origin from the gastroduodenal artery Origin from an aberrant proper hepatic artery (arising from the superior mesenteric artery) Downloaded by: University of Michigan. The regular intrahepatic bile ducts are all the time smaller than the accompanying portal vein branches. The proper and left hepatic ducts can be defined with ultrasound and are approximately 2 mm in diameter. Dilatation of the intrahepatic bile ducts is characterised initially by a unilateral thickening of the periportal connective tissue. Gallbladder volume is measured sonographically in the fasting state and once more after stimulation. Volume dedication is based on the belief of a rotational ellipsoid using a simplified geometric formula: Volume � 1 � Length � Width � Height 2 calcification.
Discount shuddha guggulu 60caps fast delivery
The testicular vein collects blood from the pampiniform plexus; it opens directly into the inferior vena cava on the best facet and into the left renal vein on the left facet. The tunica albuginea that encloses the testis appears as a thin, hyperechoic line upon the testis. The scrotal cavity, with its thin echo-free fluid rim, is most clearly visible on the head of the epididymis. The head of the epididymis, like the epididymis as an entire, is isoechoic or slightly hypoechoic and has a slightly coarser echo texture than the testis. Differentiation of the testis and epididymis is most easily completed in longitudinal scans. The tunica albuginea is most clearly depicted on T2 W images as a thin, hypointense band surrounding the testis. The epididymis is barely extra heterogeneous than the testis, showing hypo- to isointense on T1 W photographs and hypointense on T2 W pictures. Note the hyperechoic tunica albuginea bordered by a small quantity of hypoechoic fluid between the parietal and visceral layers of the tunica vaginalis (arrow). The wedge-shaped function at higher left is the top of the epididymis (triangle), which is less echogenic than the testis and shows a barely coarser texture. The tunica albuginea enclosing the testis appears as a linear hypointensity (thin arrow). The mediastinum testis with the rete testis (thick arrow) types a hypointense connection between the testis and epididymis. The head of the epididymis (star), tail of the epididymis (triangle), and spermatic cord (circle) are clearly visualized. The testis and epididymis are poorly differentiated from each other on T1 W photographs, as both seem hypointense. An undescended testis may also be situated within the abdomen or at ectopic sites outdoors the traditional observe of descent. Failure of a testicle to descend in the course of the first 12 months of life might lead to infertility as a end result of the intra-abdominal body temperature is higher than the scrotal temperature. This temperature differential also will increase the chance of growing testicular cancer. Normally the testis descends by way of the inguinal canal and into the scrotum during the 36th week of gestation. Cryptorchidism is a situation in which the testis remains undescended or maldescended, causing it to be absent from the scrotum. An incompletely descended testis is usually within the inguinal canal and can full its descent in the course of the first year Key factors. Idiopathic varicocele results from incompetent venous valves and is a frequent cause of infertility. A secondary varicocele is caused by hampered venous return in the testicular vein due to a rise of retroperitoneal pressure. Ultrasound scans ought to be performed in each the standing and supine positions and should embrace a Valsalva maneuver. The septa permeating the testis and the mediastinum testis (arrow) seem hypointense on this paracoronal T2 W picture. The head of the epididymis (triangle) and the spermatic cords (circles) within the inguinal canal are additionally clearly displayed. Scans at that stage will show a quantity of dilated, tortuous veins greater than 2 to three mm in diameter within the spermatic twine and around the epididymis. Blood flow in the affected area may be very gradual and could be detected by color duplex sonography at delicate settings. The inner spermatic vein is classed into completely different anatomical types based mostly on the presence of collateral vessels to renal capsular vessels, lumbar veins, or the inferior vena cava. The collaterals are visualized throughout interventional remedy by injecting contrast materials into the left renal vein or by selective catheterization. The presence of collaterals will determine the risk of reflux of sclerosant and the chance of recurrence after interventional sclerotherapy. Most varicoceles are asymptomatic and are sometimes detected incidentally in a morphologically normal scrotum. They are extra frequent on the left aspect because the testicular vein drains at a 90� angle into the left renal vein. These circumstances can be treated by interventional sclerotherapy with access by way of the (right) widespread femoral vein and selective catheterization of the left testicular vein.