Pariet dosages: 20 mg
Pariet packs: 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

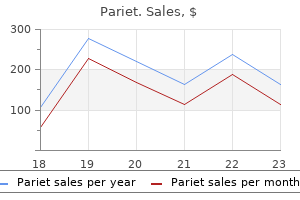
Order pariet australia
Norrie illness (retinal dysplasia) Rare X-linked recessive syndrome related to bilateral leukokoria and microphthalmia, retinal malformation, deafness, and mental retardation or deterioration. Rare autosomal recessive disorder consisting of bilateral leukokoria and microphthalmia, congenital unilateral or bilateral retinal nonattachment, profound mental retardation, lissencephaly, hydrocephaly, and with death in infancy. A contrast-enhancing cone-shaped central retrolental intravitreal density is thought to characterize the persistence of fetal tissue in Cloquet canal. Comments Rare ocular malformation with persistence of assorted portions of the primary vitreous with hyperplasia and in depth proliferation of the related embryonic connective tissue because of incomplete regression of embryonic ocular blood supply in Cloquet canal. It can replicate an isolated congenital defect or a manifestation of extra extensive ocular or systemic involvement. Presents at birth or in infancy with leukocoria (it is the second most common reason for leukocoria), poor vision, and a small eye. Retrolental fibroplasia often manifests in untimely infants who obtained supplemental oxygen remedy after delivery. Lenticular and/or choroidal dystrophic calcifications are rare however could happen within the late stage of the illness. There may be associated thickening of Tenon capsule (sclerotenonitis), serous retinal detachment, disk swelling, or serous choroidal detachment. The uveoscleral coat may be thickened and show elevated distinction enhancement (focal enhancement with abscess). Scleritis may be bacterial, fungal, or viral in origin, an idiopathic scleral inflammation, or related to systemic illness (autoimmune problems: rheumatoid arthritis, polyarteritis nodosa, relapsing polychondritis; other connective tissue illnesses; metabolic circumstances. Refers to an intraocular infectious or noninfectious inflammatory process predominantly involving the vitreous cavity or anterior chamber. Organisms: staphylococci, streptococci, meningococci, gram negatives, helminthic parasite, and cysticercosis. Comments Uncommon, often bilaterally ocular infection of youngsters (average age 6 y) in close contact with canines. The second-stage larva of Toxocara and the death of the larva lead to a wide spectrum of intraocular inflammatory reactions (granuloma, abscess, and diffuse inflammatory infiltration of the choroids and sclera). Imaging findings of toxocariasis may be just like these seen in Coats illness and noncalcific retinoblastoma. Ocular toxocariasis (sclerosing endophthalmitis) Benign neoplasms Choroidal (cavernous) hemangioma May present in two completely different forms: As a circumscribed or solitary kind, usually situated posterior to the equator of the globe within the juxtapapillary or macular region of the fundus. The lenticular, stable soft tissue mass within the wall of the globe demonstrates intense distinction enhancement. May involve as a flat, intensely enhancing mass the three components of the uvea and, often, nonuveal tissues, such as the episclera, conjunctiva, and limbus. Choroidal osteoma (choriostoma) appears as a sharply demarcated, flat, platelike calcified thickening of the posterior choroids, typically within the juxtapapillary region. Small flat or minimally elevated lesion situated most often in the posterior third of the choroid. May present as a well-defined tumor with reasonable distinction enhancement arising from the ciliary body behind the iris, encroaching upon the lens. Tends to happen within the ciliary body and peripheral choroidal area quite than in the posterior choroids. Uveal schwannoma usually impacts the ciliary physique and peripheral choroids somewhat than the posterior choroids. The tumor seems as a solitary, well-defined, oval lesion, isodense with respect to the brain, with distinction enhancement. Congenital vascular hamartomas, sometimes seen in middle-aged to aged people; isolated ocular discovering or in affiliation with neurocutaneous syndromes. Cavernous hemangiomas of the choroids are very uncommon, nonprogressive, benign lesions. Choroidal osteoma Rare benign choroidal tumor consisting of mature bone, found predominantly in otherwise wholesome younger ladies ages 10 to 30 y; 25% are bilateral, 15% multifocal.
Buy pariet now
Most colon accidents may be managed safely with main repair or resection and primary anastomosis. Small rectal injuries may be managed by major restore, and huge injuries require a proximal colostomy. The most common problems are belly sepsis (intra-abdominal abscess, wound sepsis) and colonic fistula. More than 20% of sufferers with colonic resection develop extreme stomach septic problems. The analysis of vascular injury should be suspected within the presence of severe hemodynamic instability or a quickly distending abdomen. The gestation age is assessed from the historical past, medical examination, and ultrasound. A fetal ultrasound performed by an obstetrician can assess the gestation age, the fetal heart price (fetal heart fee can be detected by 7�8 weeks) and consider for potential placenta abruption. Cardiotocography (monitoring of the fetal coronary heart fee and uterine contractions) ought to be initiated as quickly as possible in instances with viable fetus. To stop this downside, the affected person or the spinal board ought to be tilted to the left by about 20 degrees. In addition it displaces the intraabdominal organs, resulting in modifications of the harm patterns and medical indicators. Pregnancy-Related Complications (a) Placenta abruption is the commonest complication and has been reported in as much as 5% of minor trauma and as a lot as 65% in major. The traditional medical presentation consists of vaginal bleeding, ache, and fetal misery. Immunoglobulin (RhoGam) ought to be administered routinely to all Rhesus-negative injured pregnant sufferers. A mini dose (50 mcg) ought to be given in early being pregnant and a regular dose (300 mcg) after the first trimester. It is normally sophisticated by acute respiratory distress syndrome and disseminated intravascular coagulopathy. The mother could additionally be compensating at the expense of the fetus with uterine vasoconstriction. Pelvic fractures in pregnancy pose particular issues and the overall fetal mortality is about 35%. It is a life-threatening situation due to excessive bleeding and instant laparotomy is indicated. Management the trauma team should include the obstetrician and a neonatologist groups. All pregnant patients should obtain supplemental oxygen, irrespective of SaO2, as a end result of the fetal hemoglobin oxygen dissociation curve is to the left of the 5. In superior being pregnant the patient or the spinal board ought to be tilted about 20 levels to the left in order to scale back the compression of the inferior vena cava by the uterus and enhance venous return. All Rhesus-negative patients should obtain R(D) Immunoglobulin, to be able to stop isoimmunization and erythroblastosis fetalis in future pregnancies. In severe trauma, with nonviable fetus (<24 weeks) no efforts must be made to stop contractions or deliver the fetus by cesarean section. Perimortem Cesarean Section this determined procedure should be carried out in instances of maternal death or imminent dying if the fetus is potentially viable (>24 weeks). The finest outcomes are achieved if the fetus is delivered inside 5 minutes of maternal death. Fetal survival with cesarean sections 15�20 minutes after maternal dying has been reported, although the incidence of hypoxic mind harm is high. Indications for Cesarean Section Cesarean section must be performed within the presence of fetal distress if the fetus is viable (>24 weeks), if 5. Newton Orthopedic injuries are found in approximately 85% of blunt trauma victims, and thus good data in their emergency care is essential. Many accidents are also acutely life-threatening or limb-threatening and have to be evaluated in an expedited style. During the primary survey, the only attention to musculoskeletal injury is acute hemorrhage management with direct stress. Clinical Examination the bodily exam is an integral part of detecting acute orthopedic accidents. Lacerations want a more detailed analysis for neurovascular damage, tendon damage, foreign our bodies, and proximity to fracture websites.
Order generic pariet on-line
The answer to this question will discover the concept of hoop stresses and how these are resisted by the ultrastructure and gross anatomical options of the meniscus. Basic science oral 2 What is the principle sort of collagen discovered in the meniscus of the knee Can you describe the microscopic association of the collagen fibres inside the meniscus and relate this to meniscal operate This again requires the candidate to draw collectively features of the microstructure of the meniscus with the mechanical functions of the meniscus. Basic science oral three What are the contributions of the meniscus to knee operate and how does it achieve these contributions This question can result in varied different discussions, starting from the kinematics of the knee to hundreds on articular cartilage and nutrition of the articular cartilage. Vascular provide Mainly from the medial and lateral genicular arteries � within the adult blood vessels penetrate the outer 10�30% of the meniscus (slightly much less penetration within the medial meniscus). Shock absorption the presence of intact menisci reduces the height forces on the articular cartilage and underlying bone from impacts by approximately 20%. Lubrication and nutrition the increased conformity of the surfaces contributes to vitamin and possibly also to the lubrication of the joint. Function the intervertebral disc varieties part of the useful spinal unit: disc, side joints, vertebral end plates and ligaments the disc should be capable of resist compression, bending, shear and torsional (rotational shear) forces Compressive forces on the disc are greater when sitting than when standing Proteoglycans resist compressive forces (resulting from body weight above disc and motion of paraspinal muscles) Collagen fibres resist tensile forces 461 Section eight: the fundamental science oral Under compression the nucleus pulposus resists the pressure by changing it in to radial forces, that are resisted by circumferential hoop stresses in the annulus fibrosus Twisting and tensile forces are resisted by the indirect association of the collagen fibres within the lamellae of the annulus fibrosus Without the stress throughout the nucleus pulposus the annulus fibrosus can buckle, impairing its mechanical properties Disc is less stiff at low masses than at excessive masses Hysteresis decreases with repeated loading, thus reducing capability to withstand further load cycles. Mechanical factors � microtrauma and macrotrauma Metabolic � raised uric acid, diabetes, and so on. Pathology20,21 Nutrition18 Nutrition is by diffusion through the avascular disc material from the vascular plexus across the annulus fibrosus and cartilaginous finish plates Nutrition may be affected by components that intervene with the vascular plexus. Changes with growing older Proteoglycan content decreases (reducing resistance to compression) Water content decreases Uniformity of nucleus pulposus decreases � fibrous areas and softer areas Load distribution becomes uneven Composition of nucleus pulposus approaches that of the internal annulus and the junction between the 2 becomes indistinct Collagen content increases Ability to stand up to hundreds diminishes. Degenerative course of in hyaline cartilage starts at the floor and ultimately leads to exposure of bone, the bone ultimately becoming polished (eburnated) There is controversy relating to the primary event; theories embrace altered proteoglycans within articular cartilage, impaired subchondral venous drainage and altered synovial biochemistry Osteoarthrosis is thought to be a failed attempt by chondrocytes to restore broken articular cartilage; an imbalance of damage and restore Chondrocytes attempt to compensate by growing their rate of synthesis the earliest options are fibrillation of articular cartilage in superficial and transitional zones, penetration of tidemark by blood vessels from subchondral bone and subchondral bone remodelling Subchondral bone cysts and peripheral osteophytes kind. Changes in articular cartilage Early adjustments Alterations in proteoglycans Decreased aggrecan focus Increased water content material the increased permeability to water throughout the matrix and decreased stiffness. Primary � no trigger identified Secondary � rheumatoid arthritis and other inflammatory arthritides, trauma, and so forth. Progressive loss of tissue Decreased anabolic response of chondrocytes 462 Chapter 22: Basic science oral core matters Modulus of elasticity and strength decreased owing to increased water content material Articular cartilage progressively misplaced. Subchondral bone changes embrace thickening of the subchondral bone by the laying down of new bone on present trabeculae and the formation of bone cysts. Diagnostic criteria Rheumatoid arthritis is defined by the presence of four of the seven diagnostic criteria established by the American College of Rheumatology: Morning stiffness >1 hour for >6 weeks Swelling of no less than three joints for >6 weeks Involvement/swelling of wrist or arms for >6 weeks Bilateral symmetrical polyarthritis for >6 weeks Rheumatoid nodules Positive serum rheumatoid factor Radiographic modifications typical of rheumatoid arthritis (periarticular erosions, osteopenia, and so on. Intermediate Involvement of synovial-lined tendon sheaths impairs tendon tour and will lead to rupture. Radiological classifications General characteristics Insidious onset of morning stiffness, joint pain (polyarthritis), symmetrical swelling of the peripheral joints, arms and feet concerned early. Differential analysis Late � characteristic posture with lack of the conventional lumbar lordosis, thoracic kyphosis, chin-on-chest deformity, flexed hips and knees Inability to perform the wall take a look at Entire spine is ankylosed Limited chest enlargement Peripheral joint involvement; normally the hips Pronounced morning stiffness Protrusion acetabuli Heterotopic bone formation Whiskering enthesis. Differs from rheumatoid arthritis in that the illness is asymmetrical and impacts giant joints greater than small joints. The illness can start with an asymmetrical inflammatory arthritis, normally of the hip, knee or ankle. Principles of administration Control synovitis and ache Rest, splintage, non-specific medicine, specific diseasealtering drugs and synovectomy Maintain joint function Drugs, physiotherapy and generally surgery Prevent deformity Physiotherapy and splintage, tendon reconstruction and soft-tissue stabilization surgical procedure Reconstruction Excision arthroplasty and joint alternative. Radiographic features in the backbone Ankylosing spondylitis Background One of the seronegative spondyloarthropathies. A generalized chronic inflammatory situation with a predilection for the sacroiliac joints and spine. More common in males than females with estimates of ratios starting from 2:1 to 10:1. Earliest vertebral change is flattening of the traditional anterior concavity of the vertebral physique (squaring due to ossification of the anterior longitudinal ligament) Erosion and fuzziness of the sacroiliac joints occur after which later sclerosis, especially on the iliac aspect of the joint, and eventually bony ankylosis and obliteration of the sacroiliac joint Ankylosis of sacroiliac joints is followed by ossification of the interspinous and interlaminar ligaments, ankylosis of the side joints, ossification of the annulus fibrosus and syndesmophyte formation. The features proceed in a cranial path and should produce a characteristic look � bamboo spine. Superficial resemblance to ankylosing spondylitis however not an inflammatory situation, the spinal pain and stiffness are hardly ever severe and blood tests are normal Other seronegative spondyloarthritides. Pathogenesis Distension of soppy tissues quite than direct destruction of fibrosis of supporting parts. Diarthrodial joints Sacroiliac joints, vertebral aspect joints, costovertebral joints (chest pains aggravated by respiration point out involvement of costovertebral joints). Fibro-osseous junctions, syndesmotic joints and tendons Affecting intervertebral discs, symphysis pubis, sacroiliac ligament, manubriosternal joint and bony insertions of enormous tendons.
Discount pariet 20mg fast delivery
Sessile osteochondroma of humerus Clinical examination, diaphyseal achalasia, incidence of malignant transformation in both, clues to malignant transformation (increase in dimension, pain, and so forth. I mentioned need to exclude infection so this led to further discussion re Ix for infected implants (bloods, imaging, bone scan timing, and so on. Further administration � re-fuse with bone graft (discussed totally different graft options) or excision arthroplasty (discussed execs and cons). It took me some time to notice that it was a specimen eliminated throughout surgical procedure for a pars defect! Asked if I knew the classification � talked about Wiltse � this was the only time in the whole examination I was requested about a classification system! If not cauda equina however acute root ache, how would you treat (wanted conservative but in addition discussion concerning the function of acute epidural/root blocks). It is a competency-based examination and so the move price will range from examination to examination relying on the usual achieved. In recent years, the speed has diversified from between 56% and 72%, with an average pass price in 2009 of 65%. Although there shall be some very clear pass/fail questions in phrases of oral and clinical exams it is rather clear that the standard is set by the candidates themselves and their friends. When one examines it soon turns into clear to the examiner what level candidates as a bunch set for themselves and people who under-achieve accomplish that in relation to their peers. It is clear, however, that the pass fee varies depending upon the standing of the examinee. The exam has existed in its present type for a number of years now and useful statistics are rising. The reason for that is multifactorial, but will relate to a trainee having the benefit of a diversified rotation with exposure to multiple facets of orthopaedic specialties and trainers and the reality that their working life is very much targeted on self-learning and critiquing whereas non-training posts are inclined to be service-based and insular. Results do range relying upon area of training and this ought to be expected in any evaluation in any other case there could be unexplained uniformity. It stays to be seen whether or not national choice will lead to a extra even spread of outcomes. Regulations Under the November 2006 Regulations all candidates have six attempts at section 1 and three makes an attempt at part 2, after which they could apply to re-enter the examination system. January 2012 regulations From January 2012 the Joint Committee on Intercollegiate Examinations will implement new laws, which is able to restrict the number of attempts on the examination. Not surprisingly, trainees from these areas have a really high first time move price. Go to the orals and provides them your finest shot, if only for the experience, as it will be much easier next time knowing what to anticipate. A frequent mistake is to dwell an extreme amount of on a perceived poor performance in a single part of the examination, permitting this to have an result on the efficiency of the remaining examination. In reality, I passed the trauma oral very properly (and additionally the opposite two orals), however failed the paeds/hands oral � the trauma oral fully unnerved me. Genuine grievances during the course of the examination may be taken up with numerous secretarial staff present or the chairman of examiners. The assumption is that emotions are running excessive at this point and that within the warmth of the second things could be mentioned that both candidate and examiner could have cause to later regret. In the previous, if a candidate had failed the long case then they might not be passed and that was that. Some candidates might have had a borderline efficiency, and a poor efficiency in a single area may be compensated for by an above-average performance elsewhere. There is a technique of inner validation and examiners will sometimes be monitored by a third get together who takes no half in the exam. This is to alert you to be in your guard for various pitfalls and hopefully avoid them. One of essentially the most annoying components of the examination up to now was hanging round afterwards for the outcomes. If candidates had been unable to wait they may cellphone a special telephone quantity later within the night for his or her results. This has all changed, and outcomes are actually despatched to the school for verification before being despatched out within the publish to candidates roughly 1 week later with the necessary paper work to reapply in case you have failed.
Buy pariet cheap online
A very helpful tip in history-taking is to take a look at the questions within the scoring systems (Oxford knee score or hip score) that are simple and yet cowl all of the functional aspects. When we practised we began with examination of a joint or a nerve by every considered one of us and discussing why every take a look at was done and its medical significance. This helped us to be slick with examination, methodically sticking to the basics and demonstrating what we all know effectively. Despite knowing your subject properly, take a second, organize your ideas and provides a properly structured reply. The examination accounts on this e-book will present a very useful basis for preparation. We additionally imagine that candidates ought to be familiar with all pictures and diagrams in Miller. A great way is to go in early to the day unit and examine, which covers most of the brief circumstances. It plugs the gaps, filling in stuff you forgot to learn, helps in verbalizing and eliminating old habits which annoy the examiners. I found group discussion and practising the examination with my colleagues extraordinarily useful, as you get immediate feedback in your performance and might enhance on it next time. It helps to develop a routine by examining one another and avoids practising on sufferers unnecessarily. I found it helpful to go and present even the usual cases to the marketing consultant � ask him to see you often while you study. Even in common trauma conferences, practise your answer, mimicking a viva state of affairs � this was an immense assist to me. It is just repeating the identical fundamental examination whatever the complexity of the case is. A good opening and closing statement covers some mistakes to a certain extent and may deliver the 5 to a magical 6. So, just put together for all the widespread matters that you determine from previous exam experience accounts. In every medical case stick to the look, really feel, move and particular tests routine. There is time constraint briefly instances, so pay attention fastidiously to what the examiner asks you as they mark you on figuring out sure problems which would possibly be usually obtrusive. Summarize the findings with only a few acceptable negative findings before stating the provisional prognosis. Prepare to discuss in regards to the investigations and options, but begin with what your most well-liked option is and why. Hoppenfeld S, Deboer P, Buckley R (2009) Surgical Exposures in Orthopaedics: the Anatomic Approach, 4th edn. Read in depth concerning the frequent problems and you should be capable of acknowledge the rare unusual ones which take a look at the breadth of your knowledge and opportunity to rating extra. Do not just point out research should you have no idea the precise authors and numbers because the examiner might have read it only lately. You are anticipated to call a vascular surgeon in case you have a child with arterial damage in supracondylar fracture, but ought to know how References 1. Instead, save your cash and focus on a quantity of core textbooks and know them properly. You will have spent quite a bit of money by the time you get to section 2 of the exam. The final thing you need is to be stored up all night by fleas, wedding ceremony events and stag dos. I made certain that I spent some household time at weekends, no less than till the earlier couple of weeks. Revising on an train bike at the gym before work also kills two birds with one stone!
DMG HCl (Dimethylglycine). Pariet.
- Dosing considerations for Dimethylglycine.
- How does Dimethylglycine work?
- What is Dimethylglycine?
- Treating autism.
- Treating epilepsy.
- Athletic performance.
- Are there safety concerns?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96832
Generic 20 mg pariet mastercard
Preliminary abdominal radiograph A preliminary digital radiograph is obtained by the radiologist immediately previous to any colonic research. If this image exhibits a appreciable amount of fecal particles, a non-emergent research can be postponed for an additional day of prep. Small and even medium volumes of particulate feces may not be detected by the scout radiograph, however. Frontal, lateral, or oblique, coned-down digital images may be obtained to higher demonstrate staple traces, small gallstones, or renal calculi. This patient with a historical past of ulcerative colitis has fulminant colitis, so-called "toxic megacolon. A pedunculated tubulovillous adenoma is demonstrated on a spot radiograph of the sigmoid colon as a three cm coarsely lobulated area (long arrows) coated by barium. Fine tumor lobules are seen en face as 1�2 mm radiolucencies outlined by barium in interstices between the nodules (arrowheads). The clean, triangularshaped pedicle of regular mucosa is recognized by quick arrows. Detection of poor anal sphincter tone indicates a single distinction enema could additionally be a simpler examination. Patient mobility can be tested by having the patient turn on the radiographic desk high. Non-latex gloves are most popular for rectal examination, as anaphylactic reactions to latex in gloves or in rectal tip balloons have been reported. Colonic leisure Use of a colonic relaxing agent makes distinction enema more snug. Intravenous glucagon permits higher colonic distention, improving radiographic detection of lesions. Rapid injection of glucagon may trigger colonic cramps, nausea, and even dry-retching. Contraindications to glucagon embrace a historical past of prior hypersensitivity reaction to glucagon, pheochromocytoma, or insulinoma. A single contrast barium examination is most popular in sufferers with colonic obstruction suspected by plain radiograph. Some surgeons choose that a affected person with a suspected high-grade obstruction receive a water-soluble distinction enema to avoid having residual barium within the colon previous to emergent surgical procedure. A barium examine is contraindicated in a affected person with suspected colonic perforation. Therefore, sufferers with suspected proximal perforation in the proximal colon should undergo a single contrast enema utilizing an iodinated distinction agent. Patients with a suspected rectal or sigmoid leak may receive a fullstrength water-soluble contrast enema by way of a Foley catheter. Patients with poor rectal tone or unable to roll 360 degrees ought to endure a single contrast examination, with both barium or water-soluble distinction, depending on the medical history. Patients with redundant transverse or right colons are harder to research with double distinction approach. Choice of examination A double contrast (air contrast) barium enema is carried out in outpatients with suspected polyps, non-obstructing carcinoma, diverticular disease, or mild inflammatory bowel disease. A double contrast examination pictures the luminal contour in profile and the mucosal floor en face. The radiologist seems for alteration of the luminal contour, including disappearance of the contour, or protrusion of the contour in to or out of the bowel. Alterations of the Enema tip insertion After being coated with lubricant, a large bore enema tip is gently inserted in to the rectum. This tip has an connected non-latex enema balloon/insufflator sponge pad to aid retention and separate wider bore blue-colored tube with air bulb to pump air in to the rectum (an air tip named for Roscoe Miller, M. We use this tip for each double and single contrast examinations and discard the large blue insufflator bulb after every use. Spot radiograph of the sigmoid colon exhibits scattered diverticula (arrowhead) and delicate circular muscle thickening. Spot radiograph of the sigmoid colon obtained with a shallow barium pool demonstrates a 1.
Purchase pariet with paypal
Methylcellulose infusion charges might vary from 50 to a hundred and fifty ml/minute, with usual infusions charges of 80�120 ml/minute. Once methylcellulose infusion commences, the radiologist displays development of the barium column via the ileum and the development of a double contrast impact extra proximally. Compression of methylcellulose-filled bowel loops is limited to forestall diffusion of the barium in to the methylcellulose column. Spot radiographs are obtained in each the one distinction and double distinction phases. Images of the primary jejunal loops and pelvic ileum should be obtained routinely during the single distinction part, as these areas could additionally be overdiluted with methylcellulose later in the examination. Compression is applied progressively as spot radiographs are obtained to limit mixing of barium and methylcellulose. In common, the jejunum is greatest seen with the patient in a proper posterior oblique position with respect to the fluoroscopic desk prime. The ileum is normally best seen with the affected person in a supine or left posterior indirect position. In some cases, pelvic ileal loops are greatest visualized with the affected person in a susceptible position whereas compression is applied with a balloon paddle. The relationship of small intestinal loops to the anterior abdominal wall is studied by turning the patient in to a lateral position. A lateral place may also be useful for visualization of loops deep in the pelvis. The glucagon relaxes the small gut, improving luminal distention and the standard of pelvic ileal images. In patients with malabsorption or gastrointestinal bleeding, the radiologist ought to image the duodenum and duodenojejunal junction at the end of the examination. The balloon of the enteroclysis catheter is deflated and the enteroclysis catheter is slowly pulled again in to the duodenum. When the catheter reaches the third portion of the duodenum, the balloon is reinflated with 3�5 ml of room air. Once the duodenum is imaged, the balloon is deflated and the catheter is quickly eliminated. Enteroclysis variants Jejunostomy tube enema the small intestine may be studied by way of a jejunostomy tube. This kind of examination is often performed to evaluate a poorly functioning jejunostomy tube, to verify for a leak, or to exclude small bowel obstruction by adhesions or intussusception associated to the jejunostomy tube. The tip of the 124 Chapter 6: Examination of the small gut: strategies and normal anatomy A B. The tip of the jejunostomy tube (thin arrow) is distal to the J-tube entry website (arrowhead). Reflux of barium retrogradely from the tip reveals a shelf-like cut-off at the J-tube entry web site. The loop (arrowhead) simply proximal to the J-tube entry website is dilated and filled with a big radiolucent filling defect (short arrows) coated by flecks of barium. Spot radiograph obtained just after several milliliters of water-soluble distinction are injected in to the jejunal tube. Injection of another 10 ml of water-soluble contrast exhibits that some distinction enters the jejunum by way of the tip of the tube. Thus, the leak happens proximal to the J-tube tip, presumptively because the J-tube enters the wall of the small intestine. Thick folds near a jejunostomy tube can be attributed to lack of washing of the succus entericus off the folds, a reaction to J-tube feeding options, or to ischemia. A B jejunostomy tube is generally distal to the site where the tube enters the small gut. Once the tube entry web site is demonstrated, the jejunostomy tube is injected with water-soluble distinction if a leak is suspected and barium if obstruction is suspected.
Trusted 20 mg pariet
Some tendons arise from deep within the muscle, allowing a multipennate association of muscle fibres; this will increase the relative power of the muscle however at the expense of vary of movement. Surrounding connective tissue the fascicles within a tendon are surrounded by loose areolar tissue � the endotenon, which permits longitudinal movement between collagen fascicles. Groups of fascicles type the tendon the collagen fibres also show crimping, a wavy appearance, which influences the mechanical behaviour of tendon materials. Composition and construction Neurovascular supply the blood supply to tendons is derived primarily by way of the musculotendinous junction, with some further communication with the periosteal vessels on the insertion In those tendons with a paratenon, blood vessels penetrate the tendon throughout its length In these tendons with a synovial sheath, the outer and inside sheaths (parietal and visceral, respectively) are linked by a mesotenon, which transmits the vessels. The mesotenon may be continuous, or it might be confined to vinculae, as within the lengthy flexors of the digits Further diet is derived from the synovial fluid, and this can be the main supply of diet for some long tendons, such as the long flexors of the fingers the blood vessels kind a community in the epitenon and then move between fascicles within the endotenon the nerve supply is derived from the corresponding muscle, and tendons contain both fast and gradual adapting sensory organs (Golgi organs, Pacinian corpuscles and Ruffini endings). Mechanical behaviour Tendons are viscoelastic structures and, like all viscoelastic constructions, they show creep, hysteresis and stress rest. Extrinsic healing is more more doubtless to produce adhesions and result in a much less satisfactory medical outcome. Ligaments Ligament structure is mostly just like that of tendons although there are some variations. Ligaments are most likely to be strongest when forces are applied parallel to their fibres and weakest when shear forces are applied at their insertions in to bone. Ligaments are viscoelastic15 and show the viscoelastic properties of creep, stress rest and hysteresis. Sprains could be divided in to three grades: Grade I sprain � partial tear disrupting a minimal of one useful band. As a result of their viscoelastic behaviour, tendons not only transmit forces but are additionally able to storing power, which improves the efficiency of the muscle�tendon unit throughout repeated excessive impact exercise. I Non-linear region: the tendon begins off comparatively non-stiff and turns into progressively stiffer with growing elongation. This region probably displays straightening out of the crimping of the collagen fibres. Haemorrhagic/inflammatory part Formation of haematoma Invasion by polymorphonuclear cells and monocytes/ macrophages with release of cytokines and progress factors Debris eliminated and replaced with fibroblasts and capillary buds. Muscle Structure Remodelling section Collagen fibres reorganize to turn out to be oriented along the lengthy axis of the tendon the fundamental muscle cell, or fibre, which is surrounded by the basal lamina. The myofibrils are mechanically related to one another by proteins, primarily desmin; the muscle fibres are surrounded by epimysium the muscle fibres, or cells, are in flip are grouped in to fascicles surrounded by a perimysium Fascicles are grouped in to a muscle surrounded by an epimysium. Secondary afferent endings (flower spray fibres), delicate to regular stage tension. These three types are often equated to gradual oxidative, fast oxidative and glycolytic, and fast glycolytic, respectively, although that is most likely not justified. Muscle contraction Muscle contraction is initiated by launch of acetylcholine at the neuromuscular junction the acetylcholine diffuses in to the synaptic clefts Muscle contraction is controlled by calcium, which is stored in, and managed by, the sarcoplasmic reticulum Calcium is transmitted in to the muscle by way of the transverse tubular system (T system) Calcium binds to troponin on the actin filaments, thus releasing the actin filament and enabling it to interact with the myosin, resulting in contraction Contraction velocity of muscle is proportional to fibre length. Types of muscle contraction Isotonic (dynamic) Muscle pressure is constant via the range of movement Muscle size modifications. Isometric (static) Muscle pressure is generated but the length of the muscle stays unchanged. Muscle spindle Isokinetic (dynamic) Muscle tension is generated as the muscle contracts at a constant velocity over a full vary of motion. Sensory structure within a muscle that regulates tension and acts as a proprioceptive organ: Primary afferent endings (annulospiral fibres), which respond primarily to the speed of change of length Concentric contraction Muscle shortens during the contraction. Eccentric contraction Muscle lengthens while contracting against an opposing drive. Muscle�tendon junction Muscle and tendon fibres are nearly parallel, which generates excessive shear forces A excessive degree of membrane folding generates a large floor area, reducing stress at the junction and reducing the angle of force vector. Specific features include: shorter sarcomere lengths, greater artificial capacity, larger variety of organelles per cell, interdigitation of the cell membrane and intracellular connective tissue. Nerve injury (Seddon) Neurapraxia Nerve contusion involving reversible conduction block without Wallerian degeneration Selective demyelination of the axon sheath. The dialogue might go on to discover viscoelastic properties in general or the relevance of the ultimate word pressure to ligament accidents in different anatomical sites.