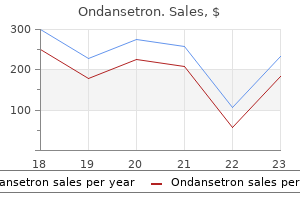
Ondansetron dosages: 8 mg, 4 mg
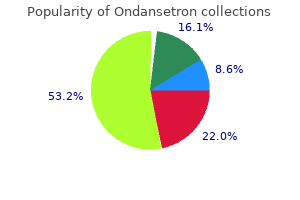
Ondansetron packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

Discount ondansetron 4 mg with amex
Intestinal endotoxemia plays a central role in development of hepatopulmonary syndrome in a cirrhotic rat model induced by multiple pathogenic factors. Multiple pathogenic factorinduced complications of cirrhosis in rats: a brand new model of hepatopulmonary syndrome with intestinal endotoxemia. Analysis of pulmonary heme oxygenase-1 and nitric oxide synthase alterations in experimental hepatopulmonary syndrome. Carboxyhemoglobin levels in cirrhotic sufferers with and without hepatopulmonary syndrome. Noradrenalin versus the mixture of midodrine and octreotide in sufferers with hepatorenal syndrome: randomized medical trial. Terlipressin is superior to noradrenaline within the administration of acute kidney damage in acute on chronic liver failure. Transjugular intrahepatic portosystemic shunt in the management of complications of portal hypertension. Renal perform after orthotopic liver transplantation is predicted by period of pretransplantation creatinine elevation. Clinical outcomes after liver transplantation for hepatorenal syndrome: a scientific review and meta-analysis. Lack of renal enchancment with nonselective endothelin antagonism with tezosentan in kind 2 hepatorenal syndrome. Sorafenib remedy improves hepatopulmonary syndrome in rats with biliary cirrhosis. Vascular endothelial development issue stimulates rat cholangiocyte proliferation through an autocrine mechanism. Potential medical targets in hepatopulmonary syndrome: lessons from experimental models. In vivo gene transfection with hepatocyte progress issue through the pulmonary artery induces angiogenesis within the rat lung. Platelet-derived progress issue is increased in pulmonary capillary hemangiomatosis. Estrogen paradox in pulmonary hypertension: current controversies and future views. Determinants of right ventricular ejection fraction in pulmonary arterial hypertension. Improved survival after liver transplantation in sufferers with hepatopulmonary syndrome. Hepatopulmonary syndrome and portopulmonary hypertension: a report of the multicenter liver transplant database. Intrapulmonary arteriovenous shunt in youngsters with persistent liver disease: clinical features, laboratory knowledge and outcome. Parenchymal alterations in cirrhotic livers in sufferers with hepatopulmonary syndrome or portopulmonary hypertension. Utility of pulse oximetry in the detection of arterial hypoxemia in liver transplant candidates. Pulse oximetry is insensitive for detection of hepatopulmonary syndrome in patients evaluated for liver transplantation. Screen for portopulmonary hypertension, particularly in liver transplant candidates. Novel presentation and method to administration of hepatopulmonary syndrome with use of antimicrobial agents. N-acetylcysteine effects on genotoxic and oxidative stress parameters in cirrhotic rats with hepatopulmonary syndrome. Hepatopulmonary syndrome efficiently handled with transjugular intrahepatic portosystemic shunt: a three-year follow-up. Use of transjugular intrahepatic portosystemic shunt as a bridge to liver transplantation in a patient with severe hepatopulmonary syndrome. Deleterious results of betablockers on train capacity and hemodynamics in patients with portopulmonary hypertension. Successful liver transplantation following medical management of portopulmonary hypertension: a single-center sequence. High brain-natriuretic peptide degree predicts cirrhotic cardiomyopathy in liver transplant patients. High fee of cardiac abnormalities in a postmortem evaluation of sufferers suffering from liver cirrhosis.
Order line ondansetron
Hepatitis G virus coinfection in liver transplantation recipients with persistent hepatitis C and nonviral persistent liver illness. Durable sequence stability and bone marrow tropism in a macaque mannequin of human pegivirus an infection. Systematic evaluation: non A-E, seronegative or indeterminate hepatitis; what is that this lethal illness Rapid metagenomic identification of viral pathogens in scientific samples by realtime nanopore sequencing evaluation. The perils of pathogen discovery: origin of a novel parvovirus-like hybrid genome traced to nucleic acid extraction spin columns. The scientific manifestations of infectious mononucleosis: a report of 2 hundred cases. Clinical manifestations and quantitative analysis of virus load in Taiwanese children with Epstein-Barr virus-associated infectious mononucleosis. Severe cholestatic jaundice induced by Epstein-Barr virus infection within the aged. Association of virus infected-T cell in severe hepatitis brought on by major Epstein-Barr virus an infection. Characterization and remedy of continual lively Epstein-Barr virus illness: a 28-year expertise within the United States. Characteristics of EpsteinBarr virus hepatitis amongst patients with jaundice or acute hepatitis. Epstein-Barr virus hepatitis: diagnostic worth of in situ hybridization, polymerase chain response, and immunohistochemistry on liver biopsy from immunocompetent patients. Lack of impact of peroral acyclovir for the treatment of acute infectious mononucleosis. Surveillance of Epstein-Barr virus hundreds in adult liver transplantation: associations with age, intercourse, posttransplant times, and transplant indications. Rituximab remedy for EpsteinBarr virus-related continual hepatitis following residing donor kidney transplantation. Transfusion-transmitted virus in association with hepatitis A-E viral infections in varied forms of liver diseases in India. Cytomegalovirus and human herpesvirus 6, however not human papillomavirus, are current in neonatal big cell hepatitis and extrahepatic biliary atresia. A case report and literature evaluate of portal vein thrombosis related to cytomegalovirus infection in immunocompetent patients. Comparison of cytomegalovirus antigenemia and tradition assays in sufferers on and off antiviral remedy. Fulminant, acyclovir-resistant, herpes simplex virus type 2 hepatitis in an immunocompetent lady. Herpes simplex virus hepatitis in infants: medical outcomes and correlates of disease severity. Herpes simplex virus hepatitis: an evaluation of the printed literature and institutional cases. Demographics and outcomes of extreme herpes simplex virus hepatitis: a registry-based study. Incidence and pure history of chemically outlined varicella-zoster virus hepatitis in youngsters and adolescents. Disseminated varicella infection in adult renal allograft recipients: four instances and a review of the literature. Parvovirus B19 induced hepatic failure in an grownup requiring liver transplantation. Acute fulminant hepatic failure associated with parvovirus B19 an infection in an immunocompetent adult. Acute fulminant hepatitis with bone marrow failure in an grownup due to parvovirus B19 infection. Co-infection of human parvovirus B19 in Vietnamese patients with hepatitis B virus infection. Intrahepatic long-term persistence of parvovirus B19 and its role in chronic viral hepatitis. Outcome of anti-thymocyte immunoglobulin plus cyclosporine A for extreme aplastic anaemia with chronic hepatitis B virus infection.
Syndromes
- Loss of menstrual period
- Primary aldosteronism
- Gagging.
- Are there pinpoint red spots?
- Convulsions (seizures)
- Withdrawal from family or friends
- Stiff neck or face
- Chemical exposure at work. About one in four cases of bladder cancer is caused by coming into contact with to cancer-causing chemicals at work. These chemicals are called carcinogens. Dye workers, rubber workers, aluminum workers, leather workers, truck drivers, and pesticide applicators are at the highest risk.
- Liver function tests
- Skin lesion biopsy
Generic ondansetron 8 mg on line
When the tumor is confined to one lobe, surgical resection is healing, even within the presence of cardiac failure. Although generally diffuse, the nodularity is sometimes focal, by which case the lesion may be mistaken for a tumor. Patients with nodular regenerative hyperplasia sometimes current clinically with portal hypertension. Partial nodular transformation is characterised by nodules that are limited to the perihilar area of the liver. Macroregenerative nodules may occur in superior cirrhosis or after large hepatic necrosis. The lesion could additionally be solitary or a quantity of and reveals a mix of chronic inflammatory cells, with plasma cells predominating. Focal fatty infiltration, or focal fatty sparing within the presence of diffuse fatty infiltration, may also be mistaken for an hepatic tumor (see Chapter 87). Larger lesions might show foci of hemorrhage or necrosis, although these options are seen less frequently than in hepatocellular adenomas. The fibrous septa typically are poorly developed, and the central scar could also be absent. The lesion is sharply demarcated from the encompassing liver tissue, which is regular, however a real capsule is absent. Individual hepatocytes are indistinguishable from those of normal liver however lack the usual wire association in relation to sinusoids, central veins, and portal tracts. Other features include heavy infiltrations of lymphocytes and, to a lesser extent, plasma cells and histiocytes. Branches of the hepatic artery and portal vein present numerous combos of intimal and easy muscle hyperplasia, subintimal fibrosis, thickening of the wall, occlusive luminal lesions, and thrombosis at instances. They are categorized into 3 primary varieties: fibrocystic diseases of the liver, cystadenomas and cystadenocarcinomas, and hydatid cysts. Fibrocystic illnesses of the liver originate from abnormal persistence or defects in the progressive transforming of the ductal plate during improvement, resulting in dilated fluid-filled areas, including hepatic and choledochal cysts, portal fibrosis, and ductal plate malformations (see Chapter 62). The cysts are usually asymptomatic and found incidentally during higher belly imaging. They happen more usually in women than in men, and their prevalence will increase with age. Symptomatic liver illness correlates with advancing age, severity of renal cysts, and renal dysfunction. The use of exogenous female sex hormones may speed up the speed of development and dimension of the cysts. The 2 polycystins are transmembrane glycoproteins that advanced and localize in the major cilium, a microtubule-based structure discovered on renal and biliary tubule epithelium and thought to act as a circulate sensor and regulator of Ca2+ inflow. This coronal T2-weighted picture shows a massively enlarged liver with quite a few bright fluid-filled cysts. Septations, papillary projections, or calcification ought to elevate suspicion of another diagnosis. If intervention is required due to signs, percutaneous aspiration and sclerosis with alcohol or doxycycline will virtually at all times ablate the cyst, but recurrence is frequent. They include clear, colorless, or straw-colored fluid and are lined by a single layer of cuboidal or columnar epithelium, resembling that of bile ducts. This process gives rise to von Meyenburg complexes (see later), which turn out to be disconnected from the biliary tract throughout development and development and dilate progressively to form cysts. Abdominal discomfort or ache, postprandial fullness, consciousness of an upper stomach mass, a protuberant abdomen, incapability to bend over, and shortness of breath could additionally be current. Severe ache may be skilled with rupture or an infection of a cyst, bleeding right into a cyst, or torsion of a pedunculated cyst. Jaundice is obvious in roughly 5% of patients and is attributable to compression of the main intrahepatic or extrahepatic bile ducts.
Best ondansetron 4mg
Information is carried out centrally by afferent neurons and peripherally by efferent neurons. It ought to be famous that in most texts, the term afferent is interchangeable with sensory. The phrases efferent and motor relating to neural provide are used to describe pathways that conduct alerts towards the "effector," in this case the small intestinal easy muscle. Although the significance of motor innervation for motility is self-evident, the pivotal role of afferent perform in determining motor responses has been much less well appreciated. The importance of the extrinsic afferent innervation in sensory signaling is emphasised by the statement that at least 80% of vagal fibers are afferent quite than efferent. The latter 2 groups may be additional subdivided into excitatory and inhibitory motor neurons and ascending and descending interneurons, respectively. Together these 3 groups type complex networks that are liable for coordinating intestinal motility. Contractions end result from activation of ascending pathways, with ascending interneurons synapsing onto excitatory motor neurons, whereas relaxations outcome from descending interneuron activation of inhibitory motor neurons. Other categories of neurons, including secretomotor and vasomotor neurons and motor neurons to endocrine cells, are recognized but not thought-about further on this chapter. Additional distinct subgroups of enteric neurons at the second are nicely characterized each structurally and functionally and are reviewed in detail elsewhere. The ganglia in the submucosal and myenteric plexuses are linked by interganglionic fascicles. The myenteric plexus consists of ganglia which may be spaced at common intervals and related by a network of interganglionic fascicles; this main community is known as the first plexus. Within this major construction, smaller branches of nerve bundles come up from the primary plexus and kind the secondary plexus, and nonetheless smaller branches form the tertiary plexus. The submucosal plexus has 2 layers, one near the mucosa and one other nearer to the circular muscle layer. The myenteric plexus also accommodates the cell bodies of intrinsic afferent neurons that discharge in response to mechanical stimulation of the muscle layer induced by muscle activity or stretch. Intrinsic afferent neurons that respond to mechanical stimulation of the mucosa are also thought to exist based on enteric reflexes seen in extrinsically denervated preparations. Current evidence means that the cell bodies of those afferents reside within the submucosal ganglia; nevertheless, this is but to be definitively described in the gut. These ileal myenteric neurons show quickly adapting responses to mechanical stimulation, whereas colonic neurons display slowly adapting responses, suggesting that these neurons can immediately encode dynamic changes in drive in response to phasic or tonic contractions. No specific neuromuscular junctions are current in small intestinal clean muscle, not like skeletal muscle, though multiple varicosities alongside the motor axons probably represent specialised areas of neurotransmission. Interneurons which have an additional sensory function have been identified, responding directly to mechanical changes in muscle length somewhat than muscle tone or pressure. Enteric glia are activated by synaptic stimulation, which suggests they play an energetic position in synaptic transmission and actively modulate physiologic intestinal processes. The anatomy of small intestinal vagal afferent innervation is relatively simple with afferent endings in the intestinal wall and cell bodies throughout the nodose and jugular ganglia, which deliver enter directly to the brainstem. These fibers then move into the thoracic dorsal ganglia and enter the spinal wire via dorsal roots, synapsing primarily on neurons of the superficial laminae of the spinal gray matter. In common, vagal afferents have decrease mechanical activation thresholds and show saturated responses at larger intensities, whereas spinal afferents are also activated at larger thresholds. The totally different stimulus response profiles of vagal and splanchnic mechanoreceptors are generally interpreted as evidence that vagal afferents regulate fullness and satiety, whereas spinal afferents mediate discomfort, bloating, and ache. Endings which have a wide dynamic range are additionally termed "muscular" or "tension" afferents and reply to round stretch however not mucosal stimulation. Wide dynamic vary afferents are activated by mechanical stimuli which are inside the physiological vary encountered during digestion. Muscular afferents show maintained responses to distention of the small gut and signal each contractile occasion, giving rise to the term in-series pressure receptors. These are in intimate contact with the connective tissue capsule and enteric glial cells that surround the myenteric ganglia, and they have been hypothesized to detect mechanical shearing forces between the orthogonal muscle layers. Its construction and the receptors and channels it expresses, nevertheless, are more probably to be distinct from those of vagal afferents, owing to spinal muscular afferents displaying greater activation thresholds to distention. These afferents are termed "muscular/mucosal" or "rigidity mucosal" in the colon and stomach, respectively, however their presence within the small gut is but to be definitively proven. Afferents with high thresholds to mechanical stimuli are noticed in the deep muscular/serosal layers and in mesenteric connections,28 and have additionally been termed "serosal" or "mesenteric" afferents.
Purchase 4 mg ondansetron mastercard
The reactivity of the activated lymphocytes spreads (epitope spread) to self-antigens distant from the original antigenic trigger, and the promiscuous activity of the activated lymphocytes can enhance inflammatory activity. The apoptotic bodies produced by these mechanisms constitute one other positive feedback loop (blue arrows) that sustains the immune reactivity. A discount within the quantity and function of Tregs has been proposed37-39 however not confirmed. Pruritus and hyperpigmentation are cholestatic symptoms that scale back the chance of the diagnosis. Hepatomegaly is the most common physical discovering, and splenomegaly could additionally be current. Emerging Biomarkers Investigative efforts have been ongoing to refine and individualize management strategies by figuring out quantifiable biological options (enzymes, gene products, metabolites, cell surface markers, cytokines, or antibodies) that may safe a analysis (diagnostic biomarkers), replicate the danger or severity of illness (predictive biomarkers), project illness consequence (prognostic biomarkers), or indicate remedy response (therapeutic biomarkers). Only the absence of laboratory or histologic findings of disease activity is a justification for withholding remedy. The dose of prednisone or prednisolone is reduced throughout this phase in a gradual trend until a upkeep degree is achieved. Within the maintenance phase, doses of medicine may be modified based on assessments of disease response and affected person tolerance. First-line treatment is continued till the standards for remission, treatment failure, incomplete response, and drug intolerance are met (light purple boxes). Therapy can then be discontinued, increased in dose, or decreased in dose in accordance with the response (light blue boxes). Responses (tan boxes) to the dose changes or drug discontinuation decide the necessity for different second-line therapies (light green boxes). The bold numbers inside the algorithm indicate the recommended sequence of therapies. Azathioprine (1 to 2 mg/kg daily) is normally introduced 2 weeks after prednisolone,one hundred ten,172 and the dose is elevated to a hundred mg daily as the dose of prednisolone is decreased. Follow-up liver tissue examination is preferred but not required to doc the histologic response. Magnetic resonance elastography is one other noninvasive test that accurately displays the stage of hepatic fibrosis as determined by liver tissue examination (see also Chapters seventy three and 80). The rapidity and completeness of the treatment response may also be predictive of outcome and must be monitored frequently. Confirmation of treatment failure warrants establishment of second-line remedy (see later). Incomplete Response An incomplete response connotes improvement within the laboratory indices of liver irritation but the response is inadequate to fulfill remission criteria. The expected rapidity of treatment response has not been codified, but sufferers who achieve laboratory and histologic remission within 6 months of remedy have a lower frequency of cirrhosis and liver failure than sufferers who require longer durations of treatment to the same endpoint. They could be managed alongside the identical algorithm as sufferers with therapy failure or nonresponse Management should be response-driven and individualized to guarantee continuous progress toward decision. Teratogenicity is a attainable complication of therapy with azathioprine,336,337 and oncogenicity is a possible complication of long-term immunosuppression. This advantage is diminished in cirrhosis, and budesonide-treated patients with cirrhosis can develop the identical range of complications related to standard glucocorticoid therapy. Drug toxicity or intolerance compels dose reduction or drug withdrawal as the initial motion Persistence or worsening of the aspect impact warrants discontinuation of the drug and management with different brokers (see later). Liver tissue examination also can provide reassurance that an optimal laboratory and histologic endpoint has been achieved and that untimely drug withdrawal has not been the premise for a subsequent relapse. Glucocorticoid withdrawal ought to be gradual and monitored intently over a period of no much less than 6 weeks. The azathioprine dose is usually maintained over the first half of the withdrawal interval and then lowered in dose by half till discontinuation in concert with the glucocorticoid. Disease exercise may be absolutely suppressed in 80% of sufferers during a 10-year interval of statement, and the long-term morbidity (azathioprine intolerance) is 7% and mortality price (death from liver disease) 2%. Ninety-four percent of re-treated sufferers have laboratory decision in 4 � 1 months, and 59% obtain histologic enchancment to normal or near-normal liver tissue in 8 � 2 months. Patients who relapse are re-treated with prednisone or prednisolone, together with azathioprine, until laboratory resolution is once more achieved (mean period, 4 � 1 months). Patients illiberal of azathioprine can be managed with prednisone or prednisolone alone in doses adjusted to preserve regular liver biochemical take a look at ranges. The dose of prednisone or prednisolone is then decreased by 10 mg, and the dose of azathioprine is decreased by 50 mg following every month of extra improvement.
Generic 4 mg ondansetron fast delivery
Digestion is mostly an enzymatic course of mediated by a quantity of courses of enzymes, which incorporates carbohydrases, proteases and peptidases, and lipases, phospholipases, and esterases. However, in some instances, for instance, the digestion of dietary fat, the breakdown process is facilitated by bodily and mechanical occasions, similar to forceful mixing and detergent (bile salt)-assisted dispersion to promote accessibility of the enzymes to their substrates. Salivary and gastric secretions include some of the digestive enzymes, but the most important among these enzymes come from pancreatic secretion. In addition to these enzymes in various secretions, there are others which may be associated with the apical membrane of the absorptive cells of the small intestine (enterocytes) that additionally take part in the digestive process. Even though some digestion happens in the mouth and abdomen prior to the entry of dietary constituents into the intestinal tract, the majority of digestion and virtually all absorption take place within the small intestine. Enterocytes, which represent the absorptive cells of the small intestine, are polarized with a half of their plasma membrane going through the intestinal lumen and the rest facing the portal circulation. Various enzymes and transporters are trafficked and recruited to these 2 membranes differentially to enable the digestive process to occur solely on the luminal side and the absorption of the dietary nutrients to happen vectorially from the lumen into blood or lymph. The mucosal floor of the small intestine is organized in massive folds, that are valvular flaps projecting into the intestinal lumen; these are known as Kerckring folds or plicae circulares. Paneth cells and stem cells are current exclusively in the crypts of the villi whereas the enteroendocrine cells, enterochromaffin cells, and Goblet cells are distributed sporadically in the upper two thirds of the villi. The apical membrane of the enterocytes is arranged in a brush-like construction, often referred to as microvilli, the purpose of which is to increase the floor area of the apical membrane; together, the Kerckring folds, villi, and microvilli improve the floor space a number of fold. In humans, the surface space of the small intestine is roughly 250 sq. meters (the dimension of a tennis court! This distinctive structure enhances the potential of the small gut for maximal digestion and absorption of dietary vitamins. The core of every villus accommodates blood vessels, lymphatic vessels, and immune cells. The terminal branches of the mesenteric artery convey oxygenated blood to the villi, the oxygen is extracted at the capillary level, and the draining venules ultimately join collectively to type the portal vein. Thus, the nutrients getting into the portal blood are made out there first to the liver for extraction and no matter remains is then made obtainable to different organs. In contrast, the lipid-soluble vitamins (constituents of dietary fats and in addition fat-soluble vitamins) are absorbed into lymphatic vessels and thus enter the thoracic duct, which then empties into the left subclavian vein. In adults on a standard food plan, less than 5% of the dietary carbohydrates, fat, and proteins is excreted within the feces. In neonates and untimely infants, nevertheless, this process is significantly much less environment friendly. These bacterially modified bile acids enter the portal circulation by diffusion and are taken up by the liver for subsequent secretion into bile. Thus, regular bile incorporates cholic acid, chenodeoxycholic acid, deoxycholic acid, and lithocholic acid, however only the primary 2 are synthesized by the liver whereas the other 2 are produced by colonic bacteria via chemical modification of the primary two. The 2 bile acids produced by the liver (cholic acid and chenodeoxycholic acid) are referred to as main bile acids, whereas the opposite 2 generated within the colon (deoxycholic acid and lithocholic acid) are known as secondary bile acids. The intestinal tract has to be prepared when the dietary parts arrive in the form of chyme from the abdomen; this contains the priming of the gut with secretions from the pancreas and liver, secretions that provide not solely the enzymes and bile salts necessary for the digestive process, but in addition bicarbonate to neutralize the acidic chyme from the abdomen. Salivary and gastric secretion is initiated with the cephalic section, triggered by the sight, scent, and even thought of meals; this phase is mediated by the autonomic nervous system. The mechanoreceptors current in vagal afferent fibers are activated by gastric distension, sending alerts to the brain with regard to meal size. The abdomen additionally secretes enzymes such as pepsin and lipase; nevertheless, these enzymes possess an optimal pH in the 4 to 5 vary, which is acceptable for the acidic situations of the luminal fluid in the stomach. When the chyme enters the duodenum, it introduces partially digested dietary carbohydrate, protein, and fats and also excessive concentrations of proton (acid pH) to the mucosal surface. The duodenum accommodates specific enteroendocrine cells, which respond to these parts in chyme and secrete hormones that affect the secretory and contractile features of abdomen, pancreas, bile duct, gallbladder, and sphincter of Oddi. Secretin is launched from duodenal and jejunal S cells (a subtype of enteroendocrine cell) in response to acidic pH. This hormone acts on parietal cells within the abdomen to cut back acid production and acts on ductal cells in the pancreas and biliary tract to stimulate bicarbonate secretion.
Weibe Senfsamen (White Mustard). Ondansetron.
- Dosing considerations for White Mustard.
- How does White Mustard work?
- Are there safety concerns?
- Coughs and colds; bronchitis; arthritis-like pain; swelling (inflammation) of the mouth, throat, and joints; and other conditions.
- What is White Mustard?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96157
Purchase 8 mg ondansetron mastercard
Wernicke encephalopathy and Korsakoff psychosis are mostly associated with alcohol use disorder and can manifest synchronously as WernickeKorsakoff syndrome. Wernicke encephalopathy is associated with neurologic abnormalities (nystagmus, extraocular palsy, ataxia, confabulation, coma) and anatomic lesions (hemorrhagic lesions within the thalamus, pontine tegmentum and mammillary our bodies, with severe harm to astrocytes, neuronal dendrites, and myelin sheaths). Korsakoff psychosis usually develops as Wernicke symptoms start to resolve and manifests as confusion and shortterm memory loss that may result in permanent brain injury. Thiamine deficiency is a major downside in both growing and developed nations, and primarily results from insufficient dietary consumption. Phosphorylated dietary thiamine is hydrolyzed to free thiamine by the action of intestinal phosphatases, that are abundantly expressed in the small intestine. These mutations result in impairment within the perform of the protein through modifications in stability, membrane concentrating on, and transport exercise. Intestinal thiamine uptake is adaptively regulated by the coinciding substrate degree. Intestinal thiamine uptake undergoes developmental regulation during early phases of life. Finally, intestinal thiamine uptake seems to be under the regulation of an intracellular Ca2+/calmodulin (CaM)-mediated pathway. There are considerable variations, nonetheless, amongst these nutritional vitamins, and solely vitamin E is an obligate dietary constituent. Their respective fat solubility influences their absorption, metabolism, excretion, and storage. Although their chemical buildings are identified, the retention of a letter naming system to distinguish them is helpful because each consists of numerous carefully related compounds with related properties. The complexity surrounding its dietary sources, requirement, and availability displays the existence of both retinyl esters ([preformed], previtamin A) and carotenoids (provitamin A), both requiring metabolic change to become energetic. Such complexity is further difficult by variations of their properties, regulatory features, and potential scientific applications. Carotenoids have 2 main roles in humans: macula pigments and natural precursors to vitamin A. Carotenoids include carotenes, with provitamin A capability and others, similar to lycopene, lutein, and zeaxanthin, without this functionality. Adequate availability of vitamin A is required for normal development and embryogenesis; nonetheless, vitamin A excess can cause teratogenesis within the first trimester of pregnancy. Sources and Recommended Daily Allowance Preformed dietary vitamin A is found in meat merchandise, dairy, egg yolk, liver, fish oils, and is fortified in margarine. Provitamin A is found in yellow, orange and green greens such as spinach, carrots, mango, and papaya, with fortification through meals colorings that comprise -carotene. Of these, only 3 are provitamin A precursors: -carotene, -carotene, and -cryptoxanthin. Preformed and pro-forms of vitamin A are absorbed in a different way within the small gut, and absorption additionally varies within the fed and fasted state. Preformed vitamin A is absorbed extra effectively than carotenes in the small intestine. Aside from differing degrees of absorption, there are also variances in regulatory mechanisms, postabsorption activity and metabolism. Vitamin A is a fat-soluble dietary constituent and is better absorbed within the presence of pancreato-biliary secretions when included into lipid micelles. Diffusion and transport-dependent mechanisms have been noted, with co-consumption of fats resulting in rapid uptake of retinol forms and secretion because retinyl esters are solubilized into chylomicrons. In the absence of dietary lipid, retinol is absorbed by way of a nonlipoprotein-dependent mechanism with secretion throughout the intestinal cell; thus absorption of vitamin A occurs in the form of both retinyl esters and free retinol. Absorption of carotenoids is variable and influenced by the complexity of the food matrix, preparation, dose, co-consumption of fiber, fats, preformed vitamin A and other carotenoids. There seems to be each concentration-dependent passive diffusion and a saturable active transporter mechanism, predominantly primarily based on -carotene. In the latter case, activity of the transporter may be dependent on the cis-transisomeric form that will compete for the transport mechanism. These esters are then incorporated into chylomicrons with other dietary lipids, which enter the systemic circulation via the lymphatic system. Although a small proportion of retinyl ester is removed by muscle, adipose, and other tissues, the bigger proportion remains within the chylomicron remnant, which enters the hepatocytes by way of an apolipoprotein E-dependent pathway. How vitamin A is transported from the hepatocyte to the stellate cell stays unknown.

Ondansetron 4 mg on-line
The singly or together relying different conditions for maintenance upon the severity of every case. In case of rigid foot, the next weeks of manipulation, early operaoperations are carried out. Illizarov approach, the totally different elements of the deformity are corrected by gradual stretching with the assistance of an exterior fixator. This technique is indicated in neglected and recurrent (after operation) circumstances of clubfoot. In this operacalcaneocuboid joint, the lateral tion, suitable wedges are taken out from side of the foot thus, resulting in subtalar, calcaneocuboid and talonavicular gradual correction of the deformity. Bursitis means inflammation of a bursa, which can be an anatomical or adventitious one. Adventitious bursa-These are bursae creating from connective tissue second ary to prolonged pressure over bony promi nences, the place no bursae previously existed. Irritative bursitis: this is caused by treated by rest, analgesia and ultrasonic excessive stress or friction with long therapy. Some circumstances need native hydro continued irritation, the sac gets cortisone infiltration. A bursa could additionally be contaminated with pyogenic, tuber cribed in the chapter of surgical infections. Most cases of irritative bursitis respond to as compound palmar ganglion which has been analgesics, rest to the half and removal of described later on this chapter. These are normally seen within the flexor ten elevated hereditary disposition (autosomal dominant). Pathology the palmar aponeurosis, a thin but robust membrane beneath the pores and skin of the palm is steady proximally with the palmaris longus tendon and distally, with the fibrous flexor sheaths covering the flexor tendons of the fingers. The characteristic early lesion is a collec tion of fibroblasts and contractile myofibrob lasts in the longitudinal fibers of the aponeu rosis in the palm or between the aponeurosis and the skin, forming a nodule. The nodules thus formed, coalesce to kind cords of fibrous tissue extending into the gentle tissues. When an attempt is made to lengthen the finger, the swollen a half of the tendon is reluctant to enter the constricted mouth of the fibrous sheath. In early circumstances, native injection of hydrocor patient fails to extend the terminal phalanx tisone is given. It could also be because of frequent repetitive movements corresponding to wringing clothes, typing, and so forth. The frequent fibrous sheath of the first dorsal compartment of the extensor retinacu lum containing the abductor pollicis longus and extensor pollicis brevis tendons is thick ened, the place it crosses the tip of the radial sty loid process. The situation is possibly analogous to set off finger, the other frequent form of tenovaginitis. Conservative remedy: In early instances, local injection of hydrocortisone along with relaxation and physiotherapy might treatment and reverse the method. Operative therapy: Longitudinal slitting open of the fibrous sheath of the concerned tendon effects compete cure. Other widespread sites embody dorsum of foot and ankle and palmar aspect of the wrist and fingers. It is the chronic inflammation of the ulnar bursa, the frequent synovial sheath that sur rounds the flexor tendons of the fingers viz. It gives rise to a swell � Immobilization of the concerned tendon ing which extends both above and beneath the sheaths in a plaster solid. Operative therapy: that is indicated, if Cause no improvement is observed after 3 or four months of conservative treatment. A comparable situation could complicate rheumatoid arthritis, without excision of all the diseased synovial membrane. The swelling typically incorporates an excess of In this condition, the median nerve is com fluid and there may be collections of small pressed as it pass through the carpal tunnel � fibrinous our bodies, referred to as melon seed our bodies the house between the flexor retinaculum and which look like sago grains. Clinical options the affected person is usually a younger grownup present ing with a painless lump. Inflammatory-Rheumatoid or tubercu � Pain is felt at the lateral facet of elbow lous tenosynovitis. If left alone signs could subside the distribution of the median nerve that spontaneously. The analgesias and antiinflammatory medicine patient notices that pain is relieved by for every week or so.
Order generic ondansetron from india
The inter-observer settlement based on histology alone was solely 46% however improved modestly (up to 71%) by together with standard clinicopathologic standards. The best results were achieved using a model that combined sure chosen histologic traits. Most essential is the temporal sample of disease evolution in relation to publicity to medicine or toxins. Using medicine corresponding to glucocorticoids or valproic acid on the time the new agent is began will increase the risk 4- to 10-fold. The sickness characteristically begins between 1 and 12 weeks (typically 2 to four weeks) after the drug is began; "sentinel signs" embody fever, pharyngitis, malaise, periorbital edema, headache or otalgia, rhinorrhea, and mouth ulcers. Erythematous reactions are ordinary and may evolve to toxic epidermal necrolysis or erythema multiforme, often with mucositis (Stevens-Johnson syndrome). Early modifications embrace neutrophilia and elevated ranges of acute-phase reactants; atypical lymphocytosis and eosinophilia could also be noted later. Other features include lymphadenopathy (16%), nephritis (6%), pneumonitis (6%), and extra extreme hematologic abnormalities (5%). Occasionally, liver damage may turn into evident properly after the offending drug is stopped, even so lengthy as 2 weeks for oxypenicillins and amoxicillin-clavulanate. Dechallenge and Rechallenge Another facet of the temporal relationship between ingestion of a drug and hepatotoxicity is the response to discontinuation of the drug, or dechallenge. Dechallenge must be accompanied by discernible and progressive improvement within days to weeks of stopping the incriminated agent. Exceptions occur with ketoconazole, troglitazone, etretinate, and amiodarone; with these agents, reactions could also be severe, and clinical recovery could also be delayed for months. Although some types of drug-induced cholestasis additionally could be extended, failure of jaundice to resolve in a suspected drug reaction often indicates an alternative diagnosis. Rarely, deliberate rechallenge may be used to verify the diagnosis of drug-induced liver disease or prove involvement of 1 particular agent when the patient has been exposed to several drugs or the advantages outweigh the risks, significantly if safer alternate options are unavailable. LiverTox is a web-based searchable database of information regarding liver damage ensuing from the use of prescription and nonprescription medication (see Drug-induced cholestasis ought to be considered if biliary obstruction has been excluded, and a liver biopsy could also be necessary. Diagnosis In the absence of specific diagnostic tests, the analysis requires scientific suspicion, a radical drug historical past, consideration of the temporal relationships between drug ingestion and liver disease, and exclusion of other problems. The objective weighing of proof for and against a person agent-causality assessment- is a probabilistic type of analysis. Rechallenge is the standard check for drug-induced liver illness but is hardly utilized in practice. The criteria for temporal eligibility embody the connection of drug ingestion to onset, course of the reaction after stopping the drug, and response to drug readministration. If that agent is an unlikely trigger and another well-known hepatotoxin is being taken, the latter is the extra probably wrongdoer. When possible, the more than likely hepatotoxin or all therapeutic agents should be discontinued. If the patient improves, the medication which are unlikely to be accountable can be rigorously reintroduced. For instance, preventable deaths from liver failure nonetheless happen from isoniazid hepatotoxicity. Drug toxicity must be thought of in circumstances of obscure or poorly defined liver illness, significantly in circumstances with combined or atypical patterns of cholestasis and hepatitis; cholestasis by which common causes have been excluded, especially in older adults; and when histologic options counsel a drug etiology. In such instances, Indications for Liver Biopsy Liver biopsy may be helpful in troublesome cases, especially when the temporal relationship between the ingestion of a identified hepatotoxic agent and the onset of liver harm is unclear. The medical group may benefit when new cases or patterns of drug-induced liver disease are adequately outlined; this benefit might persuade the clinician (but not always the knowledgeable patient) to proceed with a liver biopsy in equivocal instances. The mostly implicated agents are acetaminophen taken in reasonable doses underneath situations of elevated risk Determination of serum acetaminophen levels may be useful in troublesome circumstances, however the outcomes may be difficult to interpret in the context of standard ingestion, as opposed to a single episode of self-poisoning. Special emphasis, due to this fact, have to be placed on prevention and early detection of liver harm as nicely as on immediate withdrawal of the offending agent. Most medicine related to drug-induced liver disease are idiosyncratic hepatotoxins, for which liver damage happens not often. Avoiding overuse of those drugs can decrease the overall frequency of antagonistic hepatic reactions; antibiotics such as amoxicillin-clavulanic acid and flucloxacillin are pertinent examples.
Generic ondansetron 8mg without a prescription
The mortality rate associated with continual nitrofurantoin hepatitis is 20%, compared with 5% to 10% with acute hepatitis. Pneumonitis, which may progress to pulmonary fibrosis, is present in 20% of affected persons and is recommended by cough and dyspnea. In patients with continual hepatitis, clinical findings (such as spider telangiectasias, hepatosplenomegaly, muscle wasting, and ascites) might counsel cirrhosis. Serum bilirubin levels are most likely to be increased in proportion to the severity of the reaction. In distinction to most kinds of acute drug hepatitis, hypoalbuminemia is commonly present. Raised serum globulin levels are seen more usually in sufferers with continual hepatitis than in those with acute hepatitis. Monitoring liver biochemical test ranges is unlikely to be useful or cost efficient. Others Methyldopa was among the many first medication associated with immunoallergic drug hepatitis. The feminine predilection, medical and laboratory changes, course, and extrahepatic options of drug allergy are much like these for nitrofurantoin. Phenytoin causes extreme acute drug hepatitis in less than one per 10,000 individuals uncovered. Some sufferers with phenytoin reactions have an individual or familial enzymatic defect that causes reduced disposal of phenytoin arene oxide,142 indicating a possible reactive metabolite in the pathogenesis of phenytoin toxicity. The mortality price within the 2000s has been much lower (13%) than in earlier publications (40%). Some deaths are brought on by liver failure, whereas others end result from severe systemic hypersensitivity, bone marrow suppression, cutaneous and renal vasculitis, or exfoliative dermatitis. Liver histology reveals hepatocytes with ground-glass cytoplasm that represents hypertrophied smooth endoplasmic reticulum. Barbiturates, together with phenobarbital, are not often related to acute hepatitis. Described instances have resembled phenytoin reactions; fever and rash are traditional, and the speed of mortality because of liver failure is excessive. Some other medicine have a sulfa moiety that differs from that of sulfonamides and that may enhance the risk of cross-sensitivity reactions; for example, extreme hepatitis with celecoxib developed in 2 women with earlier sulfonamide sensitivity. The liver biochemical test profile is principally hepatocellular, however combined or cholestatic reactions can happen. Other shows include chronic hepatitis with autoimmune options and granulomatous hepatitis. Immune checkpoint inhibitors are an rising group of medication that have been associated with acute hepatitis. These agents reactivate T-cell exercise in opposition to cancer cells by blocking cytotoxic T-lymphocyte-associated antigen four The medical spectrum extends from asymptomatic aminotransferase elevations to severe acute hepatitis, together with deadly hepatic failure in 0. The severity of the presentation dictates administration, which ranges from momentary cessation of the offending drug in mild cases to everlasting discontinuation and use of high-dose glucocorticoids and/or immunosuppressive agents similar to mycophenolate mofetil in severe circumstances. Disulfiram (Antabuse) not often has been related to acute hepatitis, often resulting in liver failure. Of the newer oral anticoagulants, ximelagatran was withdrawn because of hepatotoxicity. Rivaroxaban and different direct thrombin antagonists have been associated with a few reviews of mainly acute hepatocellular or blended hepatocellular-cholestatic injury, with decision in most cases. Acebutolol, carvedilol, labetalol, and metoprolol have all been associated with acute hepatitis, a few of which had been extreme; some cases have been confirmed by rechallenge. The calcium channel blockers nifedipine, verapamil,160 diltiazem,161 and amlodipine162 have good security data, but uncommon circumstances of acute hepatitis with a brief incubation interval (5 days to 6 weeks) and other features of immunoallergy have been reported. Liver histology showed marked cholestasis in each cases and an inflammatory infiltrate and eosinophils in a single case.