Carbidopa dosages: 300 mg, 125 mg, 110 mg
Carbidopa packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

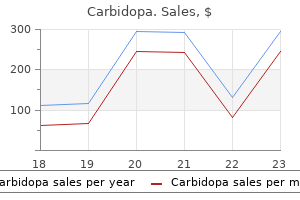
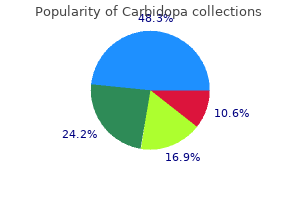
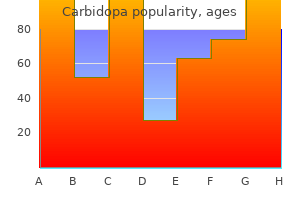
Cheap 300mg carbidopa with amex
Minimise dead-legs and blind ends in water systems, but within the unique design and because the systems are modified. Consider "no-hands" operation of utilities (for example, sensor taps, automatic lights, motion sensors for toiler flushes etc). Encourage desired behaviour (for instance, tidiness, hand hygiene) Provide enough space in all areas to enable for straightforward movement � including motion of kit and provides. Ensure correct segregation and administration of waste, together with scientific waste from linen. Provide sufficient area for storage and preparation of cleansing tools and supplies, each for cleansing employees and ad-hoc use by non-cleaning staff. Page seventy four Common Pitfalls There may be stress to choose the most cost effective merchandise or design. Design that leaves the constructing uncovered to pointless contamination, or which inspires poor apply, will value more ultimately. Clean to soiled workflows must be incorporated to make certain that the staff can practice safely and dangers are reduced. Hand wash facilities must be designed for function and conform to the full guidance i. No overflow No plug Made from non-scratch material similar to porcelain Elbow operated or no touch sensor faucets. Sink, large sufficient to enable enough room for correct hand washing to happen and curved to avoid splashing Suitably sited, foot operated waste bins and wall mounted dispensers for approved hand hygiene merchandise. Placement of hand hygiene products shall be discussed with Infection Control Suitably sited wall mounted dispensers shall be out there for disposable paper towels in an approved presentation Have a sealed waterproof back splash to allow efficient cleansing of all surfaces. Design and Cleaning For certain microorganisms, together with Clostridium difficile, cleansing performs a key position in managing outbreaks. Good design could make cleansing immeasurably easier: Use sturdy finishes that resist staining, but which are additionally simple to clean. Page 75 Where gadgets must be removed for cleaning (for example, curtains, radiator covers, ventilator grilles), make removing and alternative easy. Ensure that each one storage areas may be simply emptied for cleaning (for instance, use trolleys inside storage bays or detachable storage baskets inside cupboards). Domestic Cupboards Sufficient lodging should be provided within the form of a separate room for cleansing tools. The size and quantity required will depend upon the activity and forms of providers offered within the area. All cleansing cabinets should have house for a slop hopper for the disposal of dirty water, a sink system to clear cleaning equipment, hand wash sink, adequate storage racks for colour coded segregation of cleansing equipment and storage amenities for replenishments. Vinyl flooring in home cupboards ought to have coving (between the ground and the wall 100mm) current. Service User Accommodation Dormitory Accommodation Bed spacing has direct implications for the prevention of infections. Sufficient area for activities to be undertaken and prevent the unfold of infections is required. Infection Control will advise on spacing and is influenced by the nature of the health care facility and the kind of care. This supplies sufferers with facilities inside their quick setting and likewise allows the bay to be used for isolation purposes throughout outbreak situations. Single Rooms Where attainable an increase within the proportion of single rooms is recommended with sufficient space for essential tools. Dirty Utility Room It is crucial that ancillary areas are of a suitable commonplace and acceptable measurement for function. The precise necessities will rely upon the use of the area, the forms of providers accessing the world and the actions that will be undertaken throughout the area. The dirty utility room should be sited in shut proximity to the place procedures are carried out and have enough house to determine the workflow from dirty to clear Separate receivers such as slop hoppers should be supplied for contaminated wastewater or blood and physique fluids.
Effective 125mg carbidopa
Scaphotrapezoid anhrilis: prevalence in thumbs undergoing trapezium excision arthroplasty and effiau:y of proorimal trapezoid excision. This compares favorably with the radiographic outcomes after the hematoma distraction arthroplasty. Tomaino Thumb Carpometacarpal Joint Implant and Resurfacing Arthroplasty � Trapeziometacarpal joint (basal joint) arthritis is a debilitating condition that most commonly impacts women in their 50s and 60s. S�20 � Ligament reconstruction and tendon interposition arthroplasty, fusion, and nonbiologic reconstruction of this joint are common strategies to treat this condition. Z0 However, the appeal of a alternative could lie with faster recovery and extra nonnal kinematics. For optimum remedy outcomes with joint replacement, normal kinematics-six levels of ~om-5hould be restored as carefully as possible. All of these activities contain increasing the breadth of grasp or forceful lateral pinch. Usually the ache is localized at the base of the thwnb on the dorsal or volar radial side of the thenar cone. A "shoulder sign" is an enlarging prominence (the results of a dorsally subluxing proximal metacarpal on the trapeziwn and metacarpal adduction) that develops with progressive illness. This is necessary as a result of any concomitant illness, such as a set off thwnb, might hamper the postoperative remedy routine and negatively affect the patient"s ultimate end result. In advanced osteoarthritis, adduction and flexion contractures tend to develop, producing. Resurfacing is an more and more engaging option in younger, more active affected person:a in whom one might prefer to keep away from trapeziectomy to remove the danger of metacarpal subsidence with time. Positioning � the affected person is positioned supine on the working table with the affected hand placed on a hand desk extension. Visualize the scaphotrapezoidal joint; if it is found to have substantial degeneration, this joint floor would want to be addressed as a part of the process. The Artelon implant is shaped similar to a T, with two wings for the dorsum of the trapezium and metacarpal, with the other half to be positioned between the fresh bone edges of the trapezium and the bottom of the metacarpal. Bioabsorbable suture anchors (with 2-0 fiberwire or equivalent) are used to hold the dorsal wings down to the bone (. Although cortical bone screws were recommended to secure the implant early on, experience has shown that screws are a frequent source of complication and may pull by way of the mesh. At the end of the surgical procedure, the patient is placed right into a thumb spica splint and will observe up in 2 weeks for suture removal and placement right into a thumb spica cast for four extra weeks. Subperiosteal launch permits the base of the metacarpal to be dislocated dorsal to the trapezium. Release the adductor pollicis if required to enable abduction of the thumb metacarpal away from the palm. Use a rongeur to take away the marginal osteophytes and flatten the joint floor of the trapezium. The alignment of the metacarpal part is parallel to the axis of the metacarpal shaft. The parts are cemented into place, the trapezium first and the metacarpal second. At 2 weeks postoperatively, the sutures are eliminated and placement into a thumb spica solid rontinues for 2 more weeks. In the case of resurfacing, therapy will give consideration to range-of-motion exercises just for postoperative weeks four to 6, advancing to thenar isometrics for weeks 6 to eight. At eight weeks postoperatively, the affected person will begin grip and pinch strengthening workout routines; the splint can be discontinued at this level. Early failures with aspheric interposition arthroplasty of t:lu: thumb basal joint. Surgical management of basal joint arthritis of t:lu: thumb, part ll: ligament reconstruction with tendon interposition arthroplasty. A research of t:lu: basal joint of the thumb: remedy of its disabilities by fusion. The position and implementation of metacarpoph~al joint fusion and capsulodesis: indications and remedy alternate options. Osteoarthritis of the trapeziomctacarpal joint: t:lu: pathophysiology of articular cartila~ degew:ration, 1: anatomy and pathology of t:lu: getting older joint. Osteoarthritis of the trapcziomctacarpal joint: the pathophysiology of articular cartilage degeneration, ll: articular wear patterns within the osteoarthritic joint.
Buy carbidopa 110mg low cost
Treatment of spastic thumb-in-palm deformity: a modified extensor pollicis longus tendon rerouting. Surgery fur cerebral palsy, part 3-dassification and operative procedures for thumb deformities. Many sufferers improved perform, but no affected person Improved from dependent to impartial functioning. Furthermore, the typical time to attain this improvement was forty eight months from analysis. The "triggering" phenomenon that so commonly happens in adults is uncommon in children. The next pulley is the oblique pulley, though some authors have described an intervening distinct second annular pulley analogous to the A2 pulley within the fingera. The radial digital nerve obliquely ~osses the tendon sheath just proximal to the At pulley, and the ulnar digital nerve runs parallel to the tendon instantly alongside the At pulley. Injury to these constructions is feasible throughout surgical launch of the At pulley, so lcnowledge of the precise anatomy is important. Note the visibly protruding nodule in the flexor pollicis longus tendon on the level of the palmar digital crease. The flexed resting posture of both the interphalangeal and metacarpophalangeal joints. The interphalangeal joint typically has full passive range of motion, whereas the metacarpophalangeal joint is fiXed in flexion. It is unclear whether conservative treatment impacts the natural historical past and whether conser� vative treatment is useful for youngsters who present with a fixed flexion posture on the interphalangeal joint (most cases). Nearly all reports of surgical remedy of trigger thumb describe complete decision of the condition in the inunediate postoperative interval with a low complication price, making surgical treatment a beautiful choice. Despite claiming a 96% "satisfactory result," the authors describe solely 25% of patients with locked. Others16 have reported enchancment in triggering with nighttime splint treatment averaging tO months, but in a series that included trigger. Preoperative Planniug � Little preoperative planning is required aside from making ready the kid medically for the surgical procedure and anesthesia and making ready the household for the surgery and early postoperative recovery period. Approach � the strategy to the At pulley is greatest carried out by way of a transverse incision in or immediately parallel to the palmar digital crease. Longitudinal incisions may cause loss of metacarpophalangeal joint mobility by scar contracture long run. The precise location of the incision is dependent upon the placement of the A1 pulley relative to the crease. Great care should be taken to avoid incising the instantly adjoining digital nerves. The retractors on each side may be adjusted proximally and distally to allow visualization of the whole A1 pulley. Longitudinal division of the A 1 pulley with a 6700 Beaver blade underneath direct visualization. Note the elliptical minimize edges of the pulley and the complete extension of the interphalangeal joint. The intact proximal and distal ends of the pulley might be sources of recurrent triggering except the complete pulley is released. The wound is infiltrated with long-acting local anesthetic with out epinephrine for postoperative analgesia. Loosely wrapped gauze (A, is covered by a loosely wrapped elastic bandage (B) and a doubled-back stockinette (C) with ample tape. Great care must be taken to maintain the dressing loose to forestall excessive swelling or even ischemia distally. Thus, while in skilled hands the entire procedure takes fewer than 5 minutes, general anesthesia or sedation is required, administered by an anesthesiologist. Proximally, fibrous bands in the thenar muscle tissue could cause persistent triggering and may be divided by a gentle unfold with a blunt scissor or hemostat in the flexor sheath after A 1 pulley division.
Cheap carbidopa 125mg with amex
Activities are steadily in~eased, with high-risk activities being restricted for up to 2 years as a end result of cryon~osis of bone brought on by cryosurgery. Formal supervised remedy is initiated at the first dressing change, typically 8 to 10 days after surgery. Protective splinting continues a complete of 6 weeks minimum after intralesional procedures and till bone healing is confirmed after arthrodesis. The native recurrence price after curettage, cryosurgery, and cementation of distal radius giant cell tumor of bone is about 20% to 25% and corrdates with delicate tissue extension. Recurrence of giant-cell tumors of the long bones after curettage and packing with cement. CctmpliC4ted syndactyly refers to the interposition of accent phalanges or abnormal bones between digits. The true incidence of syndactyly is wlk:nown, partly be� explanation for the difficulty distinguishing gentle easy syndactylies from normal internet spaces. Simple incomplete syndactylies of the bilateral third web areas, with the left hand extra severely affected. Simple full syndactyly of the second and third internet areas is seen in another affected person. Local skin �laps must be used to r&:reate the couunissure to avoid scar contracture and "net creep. Judicious defatting of the pores and skin flaps should be perfonned to facilitate pores and skin closure, reduce tension throughout the flaps, and enhance the aesthetics of the reconstructed fingers. Positioning � the patient is positioned supine with the affected limb sup� ported on a hand desk. Dorsal skin flaps are most well-liked for commissure reconstruction, because of their pliability and talent to recreate the normal dorsal-proximal to volar-distal slope of the online. These flaps often are customary to traverse between the midlines of the syndactylized digits. Note the easy complete syndactyly between the index and lengthy fingers and a posh full syndactyly between the long and ring fingers. The dorsal skin flap measures roughly two thirds the size of the proximal phalanx. A non-adherent gauze bolstered with moist cotton is then positioned into the newly shaped internet house, making use of gentle compression to the skin graft sites. Reconstnldion of the Paronychium � In circumstances of simple full syndactyly, the nail plates of the involved digits are conjoined, a phenomenon generally identified as synonychia. Although division of the midportion of the nail plate is easily performed, care have to be made to reconstitute the nail folds. In "graftlessH techniques, nonetheless, dorsal skin is raised from the dorsum of the hand and advanced to recreate the interdigital commissure. The ensuing defect is dosed primarily in the style of a V-Y advancement flap (. Because proximal skin is used to recreate the web, extra tissue is on the market to permit for major closure of the digits following even handed defatting of the flaps, obviating the necessity for skin grafting. The use of preoperative tissue enlargement to keep away from the necessity for pores and skin grafting for syndactyly release has been proposed. Multiple flap designs have been proposed, and, normally, all are variations of double opposing Z-plarties1" sixteen (. In these situations, transient postoperative cart immobilization is recommended till skin flaps have healed. This is troublesome to assess within the younger youngster; however, harvest lateral to the femoral artery can function a useful information. No~ adherent gauze with appropriate bolsters placed over the pores and skin grafts and deep into the reco~ structed commissure will optimize skin graft �take� and reduce the danger of re-syndactylization through the healing period. Satisfactory useful and aesthetic results have been seen in most sufferers, but eight sufferers demonstrated net creep and three sufferers developed scar contractures. The need for secondary surgery was related to operations performed earlier than the age of 18 months, using split-thickness skin grafts, and the presence of complicated or sophisticated syndactyly. Other components which will contribute to internet creep include inappropriate flap design for commissure reconstruction, the usage of split-thickness quite than full-thickness sJcin grafts, pores and skin graft loss, and creation of a transverse linear scar in the reconstituted net area. Correction of syndactyly utilizing a dorsal omega flap and two lateral and volar flaps.
Cheap carbidopa 110mg on-line
Epilepsy Behav 2:85�91, 2001 Alper K, Devinsky O, Perrine K, et al: Nonepileptic seizures and childhood sexual and bodily abuse. Neurology 43:1950� 1953, 1993 Alper K, Devinsky O, Perrine K, et al: Psychiatric classification of nonconversion nonepileptic seizures. Biol Psychiatry 62:345�354, 2007 Alper K, Kuzniecky R, Carlson C, et al: Postictal psychosis in partial epilepsy: a case-control examine. Ann Neurol 63:602�610, 2008 American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders, 4th Edition, Text Revision. Neurology seventy five:335�340, 2010 Angeleri F, Majkowski J, Cacchio G, et al: Posttraumatic epilepsy danger elements: one year potential study after head harm. N Engl J Med 338:20�24, 1998 Arif H, Buchsbaum R, Weintraub D, et al: Patient-reported cognitive unwanted effects of antiepileptic medication: predictors and comparability of all generally used antiepileptic medication. Epilepsy Behav 14:202�209, 2009 Asikainen I, Kaste M, Sarna S: Early and late posttraumatic seizures in traumatic mind damage rehabilitation patients: brain harm factors causing late seizures and affect of seizures on long-term end result. Epilepsia forty:584�589, 1998 Bauer G, Trinka E: Nonconvulsive status epilepticus and coma. J Oslo City Hosp 28:77�86, 1978 Kotsopoulos I, de Krom M, Kessels F, et al: Incidence of epilepsy and predictive factors of epileptic and non-epileptic seizures. Am J Neuroradiol 23:218�224, 2003 Levy M, Berson A, Cook T, et al: Treatment of agitation following traumatic brain damage: a review of the literature. Epilepsy Behav 12:200�204, 2008 Luciano D: Partial seizures of frontal and temporal origin, in Neurologic Clinics, Epilepsy I: Diagnosis and Treatment. Sports Med 25:131� 136, 1998 Nadkarni S: Pitfalls in diagnosing epilepsy: a case report. Acta Neurochir Suppl ninety three:27�34, 2005 Perucca E: Clinically related drug interactions with antiepileptic medication. Ther Drug Monit 18:581�585, 1996 Pompili M, Girardi P, Tatarelli R: Death from suicide versus mortality from epilepsy in the epilepsies: a meta-analysis. J Clin Psychiatry 53:160� 162, 1992 Profitlich T, Hoppe C, Reuber M, et al: Ictal neuropsychological findings in focal nonconvulsive standing epilepticus. Epilepsia forty four (suppl 9):111, 2003 Riggio S: Psychiatric manifestations of nonconvulsive standing epilepticus. Neurology 35:1406�1414, 1985 Sarah O: Review of the function of anticonvulsant prophylaxis following mind damage. J Clin Neurosci eleven:1�3, 2004 Sengoku A, Toichi M, Murai T: Dreamy states and psychoses in temporal lobe epilepsy: mediating role of affect. Psychiatry Clin Neurosci 51:23�26, 1997 Sharpe D, Faye C: Non-epileptic seizures and child sexual abuse: a critical evaluation of the literature. Ann Gen Psychiatry 27:19, 2008 Tarulli A, Devinsky O, Alper K: Progression of postictal to interictal psychosis. Lancet Neurol 6:29�38, 2007 Thapar A, Kerr M, Harold G: Stress, anxiousness, melancholy, and epilepsy: investigating the relationship between psychological factors and seizures. Genetic factors can also contribute (Jordan 2007), though evidence concerning the apolipoprotein E genotype is somewhat mixed. Over the course of restoration, complications in relation to mood, pain, and sleep disturbance can additionally be anticipated to affect cognitive standing. This happens as a outcome of the damage incurred-both focal and diffuse-is concentrated in the anterior regions of the brain (Gentry et al. While discrete focal lesions might produce traditional neurobehavioral syndromes such as aphasia, these are commonly superimposed on the more global dysfunction ensuing from diffuse harm. Particular implications for rehabilitation and psychosocial/functional recovery are related to impairments in every area. The similarity between mild and more severe brain injury can be considered, as the two represent totally different places on a continuum of cerebral involvement (Levine et al. During posttraumatic amnesia, patients may reveal impaired consciousness and wandering consideration, whereas lack of ability to focus for more than a few minutes and distractibility characterize the early phases of recovery (Katz 1997). Because consideration underpins all features of cognition, even mild impairments can prohibit other processes such because the capability for brand new studying. Commonly reported signs include psychological slowing, trouble following conversation, lack of practice of thought, and problem attending to two issues without delay. These parts mirror the interactions of several extensively dispersed networks (Raz and Buhle 2006). For instance, a community for selective consideration has been described that includes the posterior parietal, dorsolateral frontal, and cingulate regions, performing in concert with parts of the thalamus, basal ganglia, and midbrain.
Carbidopa 125 mg on-line
Perceptual disturbances are widespread and may take the form of both illusions or hallucinations; visible (and often tactile) hallucinations strongly counsel delirium, though auditory hallucinations or illusions also occur in delirium. Suspiciousness and persecutory delusions are common, however the latter usually are poorly shaped and never well systematized, typically incorporating lots of the caregivers into the delusional ideation. Delusions need to be distinguished from confabulation in response to reminiscence deficits. Patients might refuse tests due to suspiciousness, thus interfering with their very own medical care. The sleepwake cycle is disrupted and fragmented throughout the 24-hour period, with napping and nocturnal arousals which are typically accompanied by nocturnal confusion and an lack of ability to distinguish nightmares or goals from reality. These signs of delirium sometimes fluctuate in severity to a point throughout a 24-hour interval, with phases of elevated lucidity alternating with more extreme impairment. This waxing and waning makes it tougher to assess the severity of delirium for brief time frames and complicates figuring out exactly when the episode has ended. Phenomenological work in delirium reveals the existence of three core domains of symptoms: "attention," "circadian," and "higher-level thinking. Further, measurement of these three domains using Phenomenology of Posttraumatic Amnesia and Posttraumatic Confusional State Weir et al. Using a rating scale created for the examine, they famous inability to sustain attention in higher than 50% of sufferers, wandering in larger than 30%, incoherent verbalizations in greater than 20%, inappropriate habits in approximately 15%, and temper swings in approximately 7%. Agitation was observed in roughly 27% of patients and aggression in roughly 11%. Motor agitation is frequent after acute mind injury and includes combativeness, truncal rocking, and arm thrashing (Levin and Grossman 1978). Also, agitation was not related to focal neurological indicators, focal frontotemporal injury, or (inferred) mesencephalic injury however was related to visual and auditory hallucinations and delusions. This parallels descriptions of hyperactive delirium from other causes when hyperactivity is extra usually associated with psychosis than hypoactivity (Meagher and Trzepacz 2000). This paralleled the sample of cognitive recovery after electroconvulsive therapy�induced delirium (Daniel et al. In 94% of these patients, memory deficits resolved earlier than disorientation; nevertheless, orientation to particular person preceded improvement in visible recognition memory, adopted by orientation to place, then to time, and, lastly, free recall (Tate et al. Thus their most delicate memory measure was actually final to enhance, and there was a lot particular person variation. This also supports the concept that a confusional (delirium) phase precedes an amnestic part. Invariant, well-rehearsed long-term reminiscence, represented by recall of date of delivery, persistently recovered first. Resolution of efficiency on a simple attention task occurred prior to or concurrently with reminiscence or executive function restoration in only about half of the circumstances, and a simple motor Go-No Go or easy cued reminiscence task recovered in over half previous to basic attention restoration. Schematic representation of the interrelationships amongst posttraumatic delirium, posttraumatic amnesia, posttraumatic confusion, and posttraumatic agitation. Delirium is the really helpful term because of its use throughout specialties of drugs and to improve consciousness that multiple etiologies apart from trauma can contribute to delirium in sufferers with traumatic brain damage. Episodic declarative memory deficits are more severe throughout disorientation than after it resolves (Levin et al. In distinction, declarative reminiscence is impaired in amnestic syndrome; is "express" (conscious); is subserved by the medial temporal lobe, hippocampus, diencephalon, and ventromedial frontal lobe; and consolidates over time (Squire 1986). This suggests a potential distinction within the neuroanatomical substrates of amnestic syndrome and delirium. The most typical causes embody drug intoxication and withdrawal (polypharmacy is common) and metabolic, cardiovascular, infectious, inflammatory, and traumatic causes. The first step in the administration of delirium is the diagnosis and therapy of those underlying etiological components that are most likely to be multifactorial in a given particular person. Risk elements predisposing to delirium Low serum albumin Advanced age, with or with out dementia Brain damage or central nervous system disease Preexisting cognitive deficits Prior episode of delirium Significant medical disease Polypharmacy Basal ganglia lesions on magnetic resonance imaging Cerebral atrophy with right-hemisphere focal lesions Apolipoprotein E4 allele status Risk Factors Factors that improve the chance of delirium are listed in Table 9�6.
Generic 300 mg carbidopa mastercard
In the earliest acute phase, education is probably the most essential intervention, although long-term prognostication is impossible. Families must know what has physically occurred to the injured family member and his or her brain, what therapies are being given and why, what may be expected over the subsequent few days and weeks, how to perceive uncommon habits. The timing of offering information is also crucial, as is judging how much data the family is able to take in. The seeds of long-term limitations are quietly planted early, but the expert clinician will know when the household is prepared to have them nurtured. Since the Nineteen Eighties, an infinite amount of informational materials (of variable quality) has been developed for families, and the Brain Injury Association of America is a wonderful resource for such supplies (see contact info within the section Brain Injury Association of America and Other Support Organizations). Support, downside solving, and restructuring can be efficient family interventions at individual, system, or community-relations levels. For example, the overwhelmed wife of a husband with a mind damage may need construction and guided downside solving in deciding tips on how to manage a family on limited sources. A giant household whose mother returns house after a mind injury could need to sit down as a gaggle and negotiate how family obligations should be reapportioned and take care of the inevitable emotions and conflicts generated by that course of. The household that feels trapped at home with an impulsive and aggressive teenage son might have assist in discovering artistic methods to maintain social relationships in the community or even the means to take vacations. This stage of intervention requires an lively therapist who is conscious of the realities of adjusting to brain injury and builds on the strengths and problem-solving capacities of the household and its individual members. Sometimes, serving to households negotiate transportation, work out a approach to pay for a chunk of kit, or discover a weekend social program for his or her child is a more wanted and effective intervention than concepts and psychological discussion. Formal remedy becomes appropriate when severe issues render the household system, or some a part of it, dysfunctional. Individual members of the family who profit from psychotherapy normally begin with points associated to mind damage however usually find yourself dealing with longer-standing private or family-of-origin 494 Textbook of Traumatic Brain Injury will start to turn into obvious that despite the fact that formal treatment is ending, complete recovery has not occurred, and the household faces the prospect of residing with a completely disabled person. This is an important time for intervention, when the therapist begins to deal with the anxieties and fears of the household. The community reintegration stage, as noted in the subsection Concentric Circles of Intervention, refers each to the person with mind damage and to the family system as they struggle to reenter neighborhood life under drastically modified circumstances. This part is the lengthiest and most tough and involves integration in two senses. First, the injured individual is completing formal remedy and is, as a lot as possible, changing into steadily reintegrated into the community. Expectations for full recovery begin to recede as the truth of permanent neurobehavioral impairment within the injured particular person becomes obvious, and the family system attempts to strike a model new, more permanent stability to permit its varied members to proceed with their own lives. There is gigantic variability during this ultimate section, which itself consists of a series of stages of internal adjustment. The particular person recovering from the damage makes an attempt to return as much as possible to a stage of maximum engagement and productiveness in the community, while the household settles into longer-term patterns and equilibrium that enable them to resume their household life cycle with an altered identity. This is when discouragement, despair, despair, and mourning start to happen, typically over the first few years after the top of rehabilitation. The crucial turning level occurs when, after all formal rehabilitation ends, the family as a system faces the problem of having the flexibility to reconstitute as an efficient and practical system with a new steadiness and identity. For example, a busy skilled couple could additionally be unable to reorganize their time and finances to care for a severely injured son who lives at residence, and that position may fall to a teenage daughter. If she becomes trapped in that function, she could stay residence after highschool and devote herself to caring for her brother, with the outcome that her own growth (college, career, boyfriends, marriage) could additionally be significantly blocked. Depending on her nature, she could both turn out to be critically depressed or sacrifice herself for the sake of the household to her longterm "detriment. The choice to intervene when the selfsacrifice is in the service of homeostasis raises troublesome countertransference and ethical issues, which have to be dealt with truthfully each by the therapist and directly with the family. Even when families do make the transition and their life cycle resumes, transitional factors can bring episodic issues. Families that were dysfunctional earlier than the harm could require formal family therapy after the damage, with the added complication of studying to regulate their family structure. This broad division, however, is beneficial in conceptualizing the nature of interventions that have to be made throughout each stage. In the acute stage, during which the primary points are survival, medical stabilization, and minimization of everlasting damage, the household typically coalesces, suspends regular routines, and orients all of its energy toward the care of the injured individual.