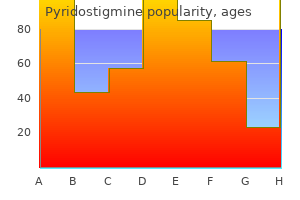
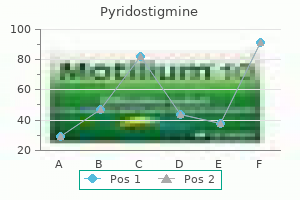
Pyridostigmine dosages: 60 mg
Pyridostigmine packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills
Order generic pyridostigmine
Patients with underlying pulmonary or cardiac disease may require higher concentrations of oxygen; oxygen therapy ought to be guided by Spo2 or arterial blood gas measurements. Patients with extreme or persistent hypoxemia must be given one hundred pc oxygen via a nonrebreathing masks or an endotracheal tube until the cause is established and different therapies are instituted; controlled or assisted mechanical air flow may be necessary. The chest radiograph (preferably with the affected person positioned sitting upright) is efficacious in assessing lung volume and coronary heart measurement and in demonstrating a pneumothorax or pulmonary infiltrates. However, in cases of pulmonary aspiration, infiltrates are often initially absent. If pneumothorax is suspected, a chest radiograph taken at end-expiration helps spotlight the pneumothorax by offering the best contrast between lung tissue and adjoining air in the pleural area. In the situation of an intubated affected person with hypoxemia, a chest radiograph provides extra usefulness to breath sound evaluation in verifying endotracheal tube position, particularly when the tube is inadvertently positioned immediately above the carina, with resultant intermittent migration into a major bronchus. An asymptomatic pneumothorax could additionally be aspirated using a intercostal catheter or adopted by remark. Diuretics must be given for circulatory fluid overload and cardiac function ought to be optimized. Bronchoscopy is usually helpful in reexpanding lobar atelectasis caused by bronchial plugs or particulate aspiration. In the setting of an intubated affected person, secretions or debris should be eliminated by suction and in addition by lavage, if necessary, and a malpositioned endotracheal tube must be appropriately repositioned. Hypotension related to sepsis and allergic reactions is normally the outcomes of each hypovolemia and vasodilation. Hypotension from a pressure pneumothorax or cardiac tamponade is the results of impaired venous return to the best atrium. Hypotension as a outcome of ventricular dysfunction is primarily encountered in sufferers with underlying coronary artery or valvular heart illness or congestive heart failure and is usually precipitated by fluid overload, myocardial ischemia, acute increases in afterload, or arrhythmias. The possibility that the circulatory abnormality is secondary to an underlying respiratory disturbance should at all times be considered before some other intervention, particularly in children. Hypotension Hypotension is usually as a result of relative hypovolemia, left ventricular dysfunction, or, much less generally, 10 excessive arterial vasodilatation. Absolute hypovolemia may finish up from insufficient intraoperative fluid replacement, persevering with fluid sequestration by tissues ("third-spacing"), wound drainage, or hemorrhage. An enhance in blood stress following a fluid bolus (250�500 mL crystalloid or 100�250 mL colloid) generally confirms hypovolemia. With severe hypotension, a vasopressor or inotrope (dopamine or epinephrine) could additionally be necessary to enhance arterial blood pressure till the intravascular volume deficit is no much less than partially corrected. Signs of cardiac dysfunction ought to be sought in patients with coronary heart illness or cardiac threat components. Failure of a patient with extreme hypotension to promptly reply to preliminary treatment mandates invasive hemodynamic monitoring, or, better nonetheless, echocardiographic examination; manipulations of cardiac preload, contractility, and afterload are often needed. The presence of a pressure pneumothorax, as instructed by hypotension with unilaterally decreased breath sounds, hyperresonance, and tracheal deviation, is an indication for quick pleural aspiration, even before radiographic confirmation. Similarly, hypotension because of cardiac tamponade, normally following chest trauma or thoracic surgery, often necessitates quick pericardiocentesis or surgical exploration. Noxious stimulation from incisional ache, endotracheal intubation, or bladder distention is usually accountable. Postoperative hypertension can also reflect the neuroendocrine stress response to surgical procedure or increased sympathetic tone secondary to hypoxemia, hypercapnia, or metabolic acidosis. Fluid overload or intracranial hypertension may also often current as postoperative hypertension. Marked hypertension can precipitate postoperative bleeding, myocardial ischemia, heart failure, or intracranial hemorrhage. Mild to average elevations can be treated with an intravenous -adrenergic blocker, corresponding to labetalol, esmolol, or metoprolol; an angiotensinconverting enzyme inhibitor, corresponding to enalapril; or a calcium channel blocker, similar to nicardipine. Hydralazine and sublingual nifedipine (when administered to patients not receiving -blockers) could cause tachycardia and myocardial ischemia and infarction. Marked hypertension in sufferers with restricted cardiac reserve requires direct intraarterial strain monitoring and should be handled with an intravenous infusion of nitroprusside, nitroglycerin, nicardipine, clevidipine, or fenoldopam. Bradycardia often represents the residual results of cholinesterase inhibitors, opioids, or -adrenergic blockers.
Diseases
- Urinary tract neoplasm
- X-linked trait
- Acute myelomonocytic leukemia
- Dystonia progressive with diurnal variation
- MASA syndrome
- Congenital sucrose isomaltose malabsorption
Buy pyridostigmine 60 mg fast delivery
The medial, lateral, and posterior cords seem as hyperechoic bundles positioned caudad, cephalad, and posterior to the artery, respectively. Three randomized, managed trials have demonstrated equivalent outcomes with a single 30-mL injection adjoining to the posterior twine or divided amongst every of the cords. Insertion of a perineural catheter should all the time be in the same location posterior to the axillary artery, and infraclavicular infusion has been shown to present superior analgesia to each supraclavicular and axillary catheters. Axillary Block At the lateral border of the pectoralis minor muscle, the cords of the brachial plexus kind giant terminal 6 branches. The axilla is also a suboptimal site for perineural catheter placement because of significantly inferior analgesia versus an infraclavicular infusion, in addition to theoretically elevated dangers of infection and catheter dislodgement. The axillary artery pulse ought to be palpated and its location marked as a reference level. Nerve Stimulation the affected person is positioned supine with the top turned to the contralateral facet, and the coracoid course of is recognized (a bony prominence of the scapula that could be palpated between the acromioclavicular joint and the deltopectoral groove). A relatively long (8 cm) insulated needle is placed perpendicular to the skin and superior instantly posterior till a motor response is elicited. An acceptable motor response is finger flexion or extension at a current less than 0. Light blue shading indicates areas of variable blockade; purple shading signifies regions of more reliable blockade. A: Use a small curvilinear probe in a parasagittal plane to visualize the brachial plexus. Transarterial Technique this system has fallen out of favor due to the trauma of twice purposefully penetrating the axillary artery along with a theoretically elevated danger of inadvertent intravascular native anesthetic injection. Nerve Stimulation Again the nondominant hand is used to palpate and immobilize the axillary artery. Once an appropriate muscle response is recognized, and after reducing the stimulation to lower than 0. Although a single injection of forty mL could additionally be used, greater success shall be seen with a quantity of nerve stimulations (ie, two or three nerves) and divided doses of native anesthetic. The axillary, musculocutaneous, and medial brachial cutaneous nerves are often spared with an axillary approach. B: A a quantity of injection method is simpler due to fascial separation between nerves. Ultrasound Using a high-frequency linear array ultrasound transducer, the axillary artery and vein are visualized in cross-section. The needle is inserted superior (lateral) to the transducer and advanced inferiorly (medially) toward the plexus under direct visualization. Ten milliliters of local anesthetic is then injected around each nerve (including the musculocutaneous, if indicated). Flexor carpi radialis Palmaris longus Flexor digitorum superficialis Flexor digitorum profundus Palmar branch Palmar digital nerves Blocks of the Terminal Nerves minal nerve, both for minor surgical procedures with a limited field or as a supplement to an incomplete brachial plexus block. Terminal nerves could also be anesthetized anyplace along their course, but the elbow and the wrist are the two most favored websites. Median Nerve Block the median nerve is derived from the lateral and medial cords of the brachial plexus. As it enters the antecubital house, it lies medial to the brachial artery close to the insertion of the biceps tendon. At the level of the proximal wrist flexion crease, it lies immediately behind the palmaris longus tendon in the carpal tunnel. To block the median nerve at the elbow, the brachial artery is identified within the antecubital crease just medial to the biceps insertion. To block the median nerve on the wrist, the palmaris longus tendon is first identified by asking the patient to flex the wrist towards resistance. Flexor carpi ulnaris Biceps tendon Flexor digitorum profundus Palmar department Dorsal department Palmar retinaculum Median n. With ultrasound, the median nerve may be recognized at the stage of the mid-forearm between the muscle bellies of the flexor digitorum profundus, flexor digitorum superficialis, and flexor pollicis longus (transducer faces perpendicular to the trajectory of the nerves). At the distal third of the humerus, the nerve moves more medially and passes beneath the arcuate ligament of the medial epicondyle. In the mid-forearm, the nerve lies between the flexor digitorum profundus and the flexor carpi ulnaris. To block the ulnar nerve at the wrist, the ulnar artery pulse is palpated just lateral to the flexor carpi ulnaris tendon.
Purchase pyridostigmine 60 mg on-line
The incision could additionally be transverse, hocky stick or horseshoeshaped over the purpose of maxi mum tenderness. Cuticular subcutaneous infections cuticular and subcutaneous an infection Treatment a. The an infection is drained via a longitudi nal web incision or distal palmar crease inci sion. In the thumb, the fibrous sheath is occupied by the tendon of the flexor pol licis longus alone. In the 4 fingers, the sheaths are occupied by the tendons of the superficial and deep flexors, the superficial splitting to spiral around the deep throughout the sheath. The proximal ends of the fibrous sheaths of the fingers obtain the insertion of the 4 slips of the palmar aponeurosis. The sheaths are sturdy and dense over the phalanges, weak and lax over the joints. The incision is placed on the free margin � Fingerseparationsign�Adjacentfingers often communicate with each other deep to it. Web house infection As the radial and ulnar bursae often com Under anesthesia a transverse skin incision is municate with one another, deep to flexor reti made and the pus is drained. The pores and skin edge is trimmed in such a means within the tendon sheaths of the little finger and the 4 slips of attachment of the palmar as to leave a diamondshaped opening to get thumb spreading proximally to the palm and forearm. Tendon sheath infection the synovial sheath of the flexor tendon is usu the skin lie the superficial and deep transverse ally infected by direct puncture wounds, par ligaments of the palm, the digital vessels and Surgical Anatomy of Flexor Tendon ticularly the place the skin is in shut contact with nerves and the tendons of the interossei and Sheath Arrangements the sheath on the skin creases however an infection might lumbricals on their method to the extensor expan additionally spread into it from adjoining lesions. The internet is filled in with a packing of fiBroUs fLexor sHeatHs Clinical Features loose fibrofatty tissue. With a big proportion of the worlds inhabitants remaining barefoot, minor pores and skin trauma is a frequent explanation for local an infection. The rising incidence of diabetes signifies that that is now a potent explanation for main infections. Local investigation with wound swabs, tradition of discharged material and pores and skin scrap ings or nail clippings may be useful in identi fyingtheorganism. Bloodinvestigationssuch as full blood rely, blood sugar and blood cultures can be helpful in determining the exact diagnosis and monitoring the benefit of treatment. Imaging � should be used to determine the extent of an infection and the buildings concerned. Treatment Treatment the essential ideas of management contain rest, elevation of foot, antibiotics and where needed, surgical debridement. Trimming the nail too 67 Section 2 Surgical Infection and Burn extreme quantities of keratin and different particles around the nail plates. Pathogenesis and Pathology the presence of poor vascularity (ischemia) and neuropathy are the two main predispos ing factors for the development of diabetic foot infections. The progress elements are released by ischemic tissues and cause endothelial cells to proliferate. The nail seems to be digging underneath the skin producing an infected tender lesion. Peripheral neuropathies this clearly predisposes the patients to unrec ognized injury, which potentiates the risk of bacterial invasion and infection. Intrinsic muscle atrophy produces tendon imbalances that expose the metatarsal heads to extreme trauma. There is a development from this superficial type of an infection by way of deep an infection and abscess formation to osteomyelitis. During routine trimming the nail is reduce straight and no try ought to be made to clip the corners. Deeper an infection might contain delicate tissue only or can involve bones (osteitis or osteomyelitis). The high incidence of internet space and toe � Deeper an infection with out abscess forma infections is said to the elevated moisture tion could be treated by strict rest, foot eleva level within the web space and the presence of tion, delicate tissue assist and antibiotics. They commonly infect the nails resulting in particularly postoperatively, the onset of fever thickening and distortion (onychogrypho or an elevated white blood cell rely may sis) which itself can lead to mechanical sign an infectious process. The commonest kind of nosocomial infection is Madura foot caused by Nocardia madurae, a filamentous organism, much like infections are as follows.
Order pyridostigmine 60 mg otc
Each patient house should be well-lighted and huge sufficient to enable quick access to patients regardless of poles for intravenous infusion pumps, a ventilator, or radiographic tools; building pointers dictate a minimal of seven ft between beds and one hundred twenty sq ft/patient. Multiple electrical shops, including no less than one with backup emergency power, and no much less than one outlet every for oxygen and suction, ought to be current at each bed house. A forced-air warming system, heating lamp, and/or a warming/cooling blanket should be out there. A readily available provide of catheters for vascular cannulation (venous, arterial, central venous) is mandatory. A defibrillation device with transcutaneous pacing capabilities, and an emergency cart with medicine and provides for advanced life support (see Chapter 55) and infusion pumps, should be present and periodically inspected. Transvenous pacing catheters; pulse mills; and tracheostomy, chest tube, and vascular cut-down trays are typically current, relying on the surgical affected person population. Appropriate gear have to be available for these sufferers requiring invasive arterial, central venous, pulmonary artery, or intracranial stress monitoring. Capnography is helpful for intubated sufferers and is increasingly employed for extubated patients as well. They should have experience in airway management and advanced cardiac life support, as well as problems generally encountered in surgical sufferers referring to wound care, drainage catheters, and postoperative bleeding. The anesthesia staff emphasizes management of analgesia, airway, cardiac, pulmonary, and metabolic problems, whereas the surgical team typically manages any problems instantly related to the surgical procedure itself. However, staffing for nursing care should be tailor-made to the distinctive caseload necessities of each facility. If the working room schedule frequently includes pediatric sufferers or frequent short procedures, a ratio of one nurse to one patient is often needed. A cost nurse ought to be assigned to ensure optimum staffing always, including the appropriate response to pressing or emergent patient care issues. Emergence from common anesthesia should ideally be characterized by a clean and gradual awakening in a managed setting. However, issues similar to airway obstruction, shivering, agitation, delirium, pain, nausea and vomiting, hypothermia, and autonomic lability are incessantly encountered. Patients receiving spinal or epidural anesthesia may expertise decreases in blood strain throughout transport or recovery; the sympatholytic results of main conduction blocks stop compensatory reflex vasoconstriction when sufferers are moved or when they sit up. As the length of anesthesia will increase, emergence additionally turns into more and more dependent on total tissue uptake, which is a function of agent solubility, the common concentration used, and the duration of exposure to the anesthetic. Recovery from most intravenous anesthetic agents depends totally on redistribution quite than metabolism and elimination. As the entire administered dose increases, however, cumulative results become clinically obvious within the type of extended emergence; the termination of action turns into more and more dependent on the metabolism or elimination. This is the premise for the concept of a context-sensitive half-time (see Chapter 7). Short and ultrashort-acting anesthetic agents, corresponding to propofol and remifentanil, significantly shorten emergence, time to awakening, and discharge. Premedication with brokers that outlast the procedure (eg, lorazepam) may be expected to prolong emergence. The quick period of motion of midazolam makes it an acceptable premedication agent for brief procedures. The results of preoperative sleep deprivation or drug ingestion (alcohol, sedatives) may also be additive to these of anesthetic brokers and may extend emergence. Delayed Emergence essentially the most frequent reason for delayed emergence (when the affected person fails to regain consciousness 30�60 min after common anesthesia) is residual anesthetic, sedative, and analgesic drug impact. Delayed emergence could occur because of absolute or relative drug overdose or potentiation of anesthetic agents by prior drug or alcohol ingestion. Less widespread causes of delayed emergence embrace hypothermia, marked metabolic disturbances, and perioperative stroke. A core temperature of lower than 33�C has an anesthetic effect and tremendously potentiates the actions of central nervous system depressants. Hypoxemia and hypercarbia are readily excluded by pulse oximetry, capnography, and/or blood fuel analysis.
Safflower Oil (Safflower). Pyridostigmine.
- What is Safflower?
- Fever, tumors, coughs, bronchial conditions, blood circulation disorders, pain, menstrual disorders, chest pain, traumatic injuries, constipation, inducing sweating, causing abortion, and other uses.
- Are there safety concerns?
- Reducing LDL cholesterol.
- How does Safflower work?
- Dosing considerations for Safflower.
- What other names is Safflower known by?
- Are there any interactions with medications?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96138
Order genuine pyridostigmine line
Tumour cells have comparatively random arrangement and monomorphic nuclei, and in such circumstances, water molecules can simply diffuse within the construction of tumour tissue. This circumstance can probably predetermine relatively high values of diffusion coefficient within the benign astrocytoma with diffuse progress. Tumour causes the destruction of pathways in some circumstances and displacement in others. T2-weighted image (a) reveals infiltrative tumour affected each white and gray matter. T2-weighted picture (a) reveals spread infiltrative and rising tumour with out clear borders, which compresses the right lateral ventricles. On T2-weighted picture (b), the sq. signifies points out the positioning of spectra taking. Thus, in an area of infiltrative progress, astrocytoma decomposes nervous fibres, while on the periphery the displacement of neighbouring pathways of white matter is especially noticed (Helton et al. Cystic degeneration and haemorrhages are sometimes noticed, but necrosis at histological examination is absent. Stages of mitosis (mitotic division) are revealed in tumoral cells and in some vessels, i. Epileptic seizures and focal neurological signs prevail within the medical picture of the disease. The prognosis for sufferers with such tumours is poor, and common life expectancy is about 2 years. Ring-shaped distinction enhancement can point to the transformation of the tumour to glioblastoma. Oedema of various degrees is usually visible across the tumour; it has low density and a typical spreading in white matter. Perifocal oedema, which has hyperintense signal and a typical form of divergent rays, could be higher visualised with the use of the same sequences. T2-weighted picture in axial (a), coronal (b) and sagittal (c) projections visualises intracranial infiltrative hyperin- tense tumour. The target biopsy of focus in the left frontal lobe established analysis of astrocytoma 354 Chapter 4. T1-weighted imaging (a,b) and T2-weighted imaging (c) show two tumours that are hyperintense (on T2-weighted image) and hypointense (on T1-weighted image). T1-weighted picture (c) with superposition of function examination data (1) demonstrates the interplay of tumour of precentral gyrus and left-sided motor centre Supratentorial Tumours 355. Tumour cysts are positioned on neoplasm convex floor 358 Chapter 4 circumstances of bigger tumour or marked oedema. Nevertheless, extra typically the focal somewhat than diffuse contrast enhancement in tumour construction is visualised. The involvement of cortical structures of the affected hemisphere is typical for the tumour. The index of partial anisotropy decreases with the increase of anaplastic changes in tumours. Infiltrative progress results in whole destruction of the principle structural components of white matter, particularly pathways (Goebell et al. Usage of tractography improves the planning of operational entry and revision of tumour resection. According to Romodanova (1965), these tumours make up 5% of all brain neoplasms in youngsters, whereas Dropcho et al. The speedy enhance of medical signs and sudden worsening due to enhance of intracranial strain and not infrequently, impaction, is observed in sufferers with this malignant tumour. Often lower than 1 month passes from the disease onset to virtually whole incapacity of the patient. The average life expectancy is about eight months; 5-year survival is observed extremely hardly ever (Lacroix et al. The central space of tumour is a zone of necrosis, with low density, seen in 95% of circumstances.
Cheap 60mg pyridostigmine otc
After distinction enhancement, an space of peripheral contrast accumulation sometimes happens, and this example requires the conducting of differential prognosis of tumours. Nevertheless, in these cases, thorough analysis of all knowledge collected during the examinations is required to avoid diagnostic errors. In the residual period, the mind tissue defect types on the site of a haemorrhage. The syndrome is clinically characterised by fast progression of neurological indicators such as headache, epileptic seizures, vision impairment, change of mentality and focal neurological signs. The growing transudation of the protein-rich interstitial liquid causes the formation of a quantity of focuses of vasogenic oedema. It is widely believed that the possible purpose could be lesser sympathetic innervation of partitions of these arteries in comparison with the walls of carotid arteries. Amyloid angiopathy, an infection, overdosing of some medicines (sympathomimetics), coagulopathy and using anticoagulant remedy are infrequent causes of intracerebral haemorrhage. However, the presumed prognosis can be made primarily based several indicators like old age with the absence of hypertension, and the presence of intracerebral (more incessantly subcortical) haemorrhages. The deposition of the particular fibrillar protein-called amyloid-in the walls of small, normally cortical leptomeningeal 3. They are accompanied by the abrupt rise of blood strain, and they quite often lead to a deadly outcome. According to published stories, the foci of petechiae, and larger cortical and subcortical haemorrhages, haemorrhages. Intracerebral haemorrhage of corti- cal and subcortical location in the proper parietal region in a 65-yearold patient with out arterial hypertension on (C) 198 Chapter 3. Unlike the haemorrhages due to arterial hypertension, the presence of a quantity of but small haemorrhages in subcortical areas of the mind is typical for amyloid angiopathy. There is some info in the literature about intracerebral haemorrhages round mind abscesses. Infectious endocarditis occurring when the contaminated blood clot meets the brain vessels, fungal vasculitis and necrotising haemorrhagic encephalitis, moyamoya disease, Rendu-Osler-Weber disease, etc. Intracerebral haemorrhage could be a complication of some drugs, similar to amphetamine and its derivatives, ephed- Cerebrovascular Diseases and Malformations of the Brain 199. The most frequent sites for the aneurysms are the websites of bifurcation, anastomosis of the basal arteries of the circle of Willis, and in rare instances, the aneurysm can type instantly from the sidewall of the non-branching artery. The aneurysmal sack could have a slender neck or wide base (or detach from an artery on a wide stalk). Twenty to 30% of all aneurysms are observed within the space of anterior cerebral� anterior communicating arteries, 10�20% on the site the place the posterior communicating artery descends from the interior carotid artery, 5�10% on the website of the interior carotid artery bifurcation, and 15�30% at the site of bi- or trifurcation of the center cerebral artery. Single aneurysms as a finding are reported in 1% of all autopsies and in 7% of all sufferers that underwent digital angiography not related to the subarachnoid haemorrhage (Nakagawa 1994; Osborn 1994; Schumacher 2000, 2002). Multiple aneurysms are observed in a fifth to a 3rd of all circumstances at intracranial places of aneurysm (Orrison 2000). About 75% of patients have two aneurysms, 15% have three and in 10%, more than three aneurysms. In cases with a quantity of aneurysms, an affiliation with gender (more regularly in women) has been observed. Multiple aneurysms are often noticed in sufferers with diseases such as vasculopathy, fibromuscular dysplasia and polycystic renal illness. Aneurysms of lateral wall-in the ostium of the posterior speaking artery, within the ostium of anterior choroid artery f. The posterior cerebral artery: the peduncular space (P1), area of the circumferential cistern (P1�P2), P2 segment, distal (P3), the superior cerebellar artery (distal segments) According to their measurement, aneurysms are divided into small (2�6 mm), intermediate (6�15 mm), giant (15�25 mm) and huge (more than 25 mm). The peak prevalence of the start of medical signs begins between the ages of 40 and 60 years. There are some distinctive attributes distinguishing aneurysms in adults from those in children. About 20% of all aneurysms in children are diagnosed in the posterior segment of the circle of Willis or within the more distal vessels. The most frequent website in youngsters as compared with the adults is the bifurcation of the interior carotid artery.
Pyridostigmine 60mg low cost
Maintenance infusion, 1�4 mg/min 150 mg over 10 min, adopted by 1 mg/min for 6 h, then 0. Potent sodium channel blocker with significant conduction-slowing effects 5�20 mcg/kg/min Hemodynamic finish factors quite than specific dose is objective. Nonselective -adrenergic blocking properties Limited by have to be infused slowly. Disposable pacing electrodes are usually positioned on the patient in an anterior�posterior manner. The placement of the adverse electrode corresponds to a V2 electrocardiograph position, whereas the optimistic electrode is placed on the left posterior chest beneath the scapula and lateral to the backbone. Failure to capture could also be as a end result of electrode misplacement, poor electrode-to-skin contact, or elevated transthoracic impedance (eg, barrel-shaped chest, pericardial effusion). Current output is slowly increased till the pacing stimuli acquire electrical and mechanical cap11 ture. Conscious patients could require sedation to tolerate the discomfort of skeletal muscle contractions. Transcutaneous pacing can present efficient temporizing remedy till transvenous pacing or different definitive treatment can be initiated. State firmly in a forceful voice the next chant before every shock: � "I am going to shock on three. If tachycardia persists, improve the joules according to the electrical cardioversion algorithm. Reset the sync mode after every synchronized cardioversion because most defibrillators default again to unsynchronized mode. This default permits a direct defibrillation if the cardioversion produces ventricular fibrillation. Data from the American Heart Association Guidelines 2010 for cardiopulmonary resuscitation and emergency cardiovascular care. In the sector, paramedics intubated the affected person, started two large-bore intravenous lines, began fluid resuscitation, and inflated a pneumatic antishock garment. Cardiopulmonary resuscitation must be initiated instantly: external chest compressions should be began as soon because the arterial blood strain is discovered to be inadequate for important organ perfusion. Pulselessness in the presence of sinus rhythm suggests severe hypovolemia, cardiac tamponade, ventricular rupture, dissecting aortic aneurysm, rigidity pneumothorax, profound hypoxemia and acidosis, or pulmonary embolism. Abdominal ultrasound can rapidly identify a collapsed vena cava, which is pathognomonic of hypovolemia. Additional venous access could be sought as different members of the operating room group administer fluid via blood pumps or other speedy infusion gadgets. The signs of rigidity pneumothorax-the presence of air underneath pressure within the pleural space-include increasing peak inspiratory pressures, tachycardia and hypotension (decreased venous return), hypoxia (atelectasis), distended neck veins, unequal breath sounds, tracheal deviation, and mediastinal shift away from the pneumothorax. Pericardial tamponade-cardiac compression from pericardial contents-should be suspected in any affected person with slim pulse stress; pulsus paradoxus (>10 mm Hg drop in systolic blood pressure with inspiration); elevated central venous strain with neck vein distention; equalization of central venous stress, atrial pressures, and ventricular end-diastolic pressures; distant heart sounds; tachycardia; and hypotension. Because external chest compressions are sometimes ineffective in trauma patients, an emergency thoracotomy ought to be carried out as soon as attainable to clamp the thoracic aorta, relieve a pressure pneumothorax or pericardial tamponade, establish potential intrathoracic hemorrhage, and carry out open-chest cardiac compressions. Cross-clamping of the thoracic aorta will increase brain and coronary heart perfusion and decreases subdiaphragmatic hemorrhage. Complications of inflating the abdominal part of the pneumatic antishock garment include renal dysfunction, altered lung volumes, and visceral harm throughout exterior chest compressions. Even then, deflation must be gradual, as it could be accompanied by marked hypotension and metabolic acidosis brought on by reperfusion of ischemic tissues. Before the recovering affected person is absolutely responsive, pain is commonly manifested as postoperative restlessness. Serious systemic disturbances (eg, hypoxemia, respiratory or metabolic acidosis, or hypotension), bladder distention, or a surgical complication (eg, occult intraabdominal hemorrhage) should also be thought-about in the differential diagnosis of postoperative agitation. These physiological effects are sometimes poorly tolerated by sufferers with preexisting cardiac or pulmonary impairment. The overwhelming majority are associated to airway obstruction, hypoventilation, and/or hypoxemia. Following naloxone administration, sufferers must be observed carefully for recurrence of opioid-induced respiratory depression ("renarcotization"), as naloxone has a shorter period than do most opioids.
Cheap 60 mg pyridostigmine otc
Increased ammonia manufacturing represents intracellular acidosis; hydrogen ions transfer intracellularly to compensate for intracellular potassium losses. The ensuing metabolic alkalosis, together with elevated ammonia production, can precipitate encephalopathy in sufferers with superior liver disease. Chronic hypokalemia has been associated with renal fibrosis (tubulointerstitial nephropathy). Treatment of Hypokalemia the remedy of hypokalemia is dependent upon the presence and severity of any related organ dysfunction. Digoxin therapy-as well as the hypokalemia itself-sensitizes the heart to modifications in potassium ion concentration. In most circumstances, the most secure technique by which to appropriate a potassium deficit is oral alternative over several days utilizing a potassium chlo7 experience solution (60�80 mEq/d). Intravenous alternative of potassium chloride is usually be reserved for sufferers with, or at risk for, significant cardiac manifestations or extreme muscle weak spot. The objective of intravenous remedy is to take away the affected person from immediate danger, to not appropriate the complete potassium deficit. Dextrose-containing options should usually be prevented as a end result of the ensuing hyperglycemia and secondary insulin secretion may actually worsen the low plasma [K+]. Potassium bicarbonate or equal (K+ acetate or K+ citrate) is preferable for patients with metabolic acidosis. Potassium phosphate is a suitable various with concomitant hypophosphatemia (diabetic ketoacidosis). The determination to proceed with elective surgery is commonly based on decrease plasma [K+] limits someplace between 3 and three. The decision, however, should also be primarily based on the rate at which the hypokalemia developed as properly as the presence or absence of secondary organ dysfunction. The latter could not apply to sufferers receiving digoxin, who could also be at elevated threat of growing digoxin toxicity from the hypokalemia; plasma [K+] values above four mEq/L are desirable in such sufferers. Intravenous potassium ought to be given if atrial or ventricular arrhythmias develop. Glucose-free intravenous solutions should be used and hyperventilation averted to forestall further decreases in plasma [K+]. When potassium consumption is increased slowly, the kidneys can excrete as a lot as 500 mEq of K+ per day. The sympathetic nervous system and insulin secretion additionally play important roles in preventing acute increases in plasma [K+] following acquired potassium loads. Hyperkalemia may end up from (1) an intercompartmental shift of potassium ions, (2) decreased urinary excretion of potassium, or, hardly ever, (3) an elevated potassium intake (Table 49�10). Measurements of plasma potassium concentration may be spuriously elevated if pink cells hemolyze in a blood specimen. In vitro release of potassium from white cells in a blood specimen also can falsely point out increased levels in the measured plasma [K+] when the leukocyte depend exceeds 70,000 � 109/L. A similar release of potassium from platelets occurs when the platelet depend exceeds 1,000,000 � 109/L. Arginine hydrochloride, which is used to deal with metabolic alkalosis, consider pituitary growth hormone reserve, and as a performance-enhancing supplement by athletes, can cause hyperkalemia because the cationic arginine ions enter cells and potassium ions transfer out to maintain electroneutrality. Hyperkalemia because of Decreased Renal Excretion of Potassium Decreased renal excretion of potassium can result from (1) marked reductions in glomerular filtration, (2) decreased aldosterone activity, or (3) a defect in potassium secretion in the distal nephron. Glomerular filtration rates lower than 5 mL/min are nearly always related to hyperkalemia. Patients with lesser degrees of renal impairment also can readily develop hyperkalemia when confronted with elevated potassium hundreds (dietary, catabolic, or iatrogenic). Hyperkalemia as a outcome of decreased aldosterone exercise may end up from a primary defect in adrenal hormone synthesis or a defect within the renin� aldosterone system. Although usually asymptomatic, these sufferers develop hyperkalemia once they increase their potassium intake or when given potassium-sparing diuretics. They also usually have various levels of Na+ losing and a hyperchloremic metabolic acidosis.
Purchase genuine pyridostigmine on line
Hebl J, Horlocker T, Kopp S, et al: Neuraxial blockade in sufferers with preexisting spinal stenosis, lumbar disk disease, or prior spinae surgery: efficacy and neurologic problems. Munnur U, Suresh S: Backache, headache, and neurological deficit after regional anesthesia. Rodgers A, Walker N, Schug S, et al: Reduction of postoperative mortality and morbidity with epidural or spinal anaesthesia: results from overview of randomised trials. Rukewe A, Alonge T, Fatiregun A: Spinal anesthesia in kids: now not an anathema. Steiner L, Hauenstein L, Ruppen W, et al: Bupivacaine concentrations in lumbar cerebrospinal fluid in sufferers with failed spinal anaesthesia. Intravenous regional anesthesia, additionally called a Bier block, can present intense surgical anesthesia for brief surgical procedures (45�60 min) on an extremity. Complete anesthesia of the knee can be attained with a proximal sciatic nerve block. In addition to potent analgesia, regional anesthesia could lead to reductions in the stress response, systemic analgesic necessities, opioid-related unwanted facet effects, common anesthesia necessities, and possibly the incidence of chronic pain. Regional anesthetics ought to be administered in an area where normal hemodynamic monitors, supplemental oxygen, and resuscitative drugs and gear are readily available. Local anesthetic may be deposited at any level along the brachial plexus, depending on the desired block effects: interscalene for shoulder and proximal humerus surgical procedures; and supraclavicular, infraclavicular, and axillary for surgical procedures distal to the mid-humerus. A properly carried out interscalene block invariably blocks the ipsilateral phrenic nerve, so cautious consideration ought to be given to patients with extreme pulmonary disease or preexisting contralateral phrenic nerve palsy. Brachial plexus block at the degree of the cords provides wonderful anesthesia for procedures at or distal to the elbow. All sciatic nerve blocks fail to present full anesthesia for the cutaneous medial leg and ankle joint capsule, but when a saphenous (or femoral) block is added, full anesthesia under the knee is offered. An understanding of regional anesthesia anatomy and techniques is required of the well-rounded anesthesiologist. The subject of regional anesthesia has accordingly expanded to one which addresses not solely the intraoperative issues of the anesthesiologist, but in addition long term perioperative ache management. Although many sufferers are candidates for regional anesthesia/analgesia, as with all medical procedure a risk�benefit analysis should be carried out. The risk�benefit ratio often favors regional anesthesia in sufferers with multiple comorbidities for whom a common anesthetic carries a larger threat. In addition, sufferers intolerant to systemic analgesics (eg, these with obstructive sleep apnea or at excessive threat for nausea) could benefit from the opioid-sparing effects of a regional analgesic. Patients with continual ache and opioid tolerance could obtain optimum analgesia with a continuous peripheral nerve block (so-called perineural native anesthetic infusion). If attainable, discussion with the surgeon about various issues (tourniquet placement, bone grafting, projected surgical duration) is ideal. Also, understanding the anticipated course of restoration and anticipated level of postoperative ache will usually influence specific choices relating to a regional anesthetic method (eg, a single-injection versus continuous peripheral nerve block). Examples embrace youthful pediatric patients and some developmentally delayed people, as properly as patients with dementia or motion disorders. Bleeding disorders and pharmacological anticoagulation heighten the chance of native hematoma or hemorrhage, and this danger should be balanced towards the attainable benefits of regional block. Specific peripheral nerve block places warranting probably the most concern are posterior lumbar plexus and paravertebral blocks owing to their relative proximity to the retroperitoneal space and neuraxis, respectively. Placement of a block needle through a website of infection can theoretically track infectious material into the physique, where it poses a danger to the goal nerve tissue and surrounding constructions. Therefore, the presence of a local an infection is a relative contraindication to performing a peripheral nerve block. Indwelling perineural catheters can function a nidus of infection; nonetheless, the chance in patients with systemic an infection stays unknown. Although nerve damage is at all times a risk with a regional anesthetic, some patients are at elevated threat.