Coversyl dosages: 8 mg, 4 mg
Coversyl packs: 10 pills, 30 pills, 60 pills, 90 pills

Coversyl 4 mg overnight delivery
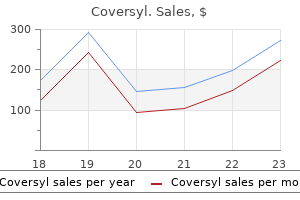
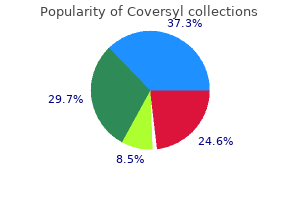
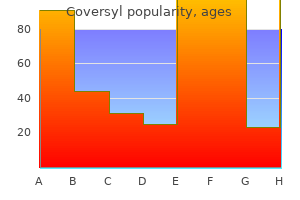
Familiarity with these new standards is crucial for radiologists and scientific neuroscientists alike. Mature cells of every sort had been as quickly as thought to bear malignant transformation, producing corresponding neoplasms. Brain tumor classification is now based on a mixture of histology and molecular diagnostics. It is powerful, reproducible, and rather more broadly out there as a surrogate for molecular genetic alterations. A number of mutant-specific antibodies are actually available and are in routine use in most main medical facilities. Histologic grading is used as a method of predicting the biologic conduct of tumors and-together with molecular features-remains an necessary guide to therapeutic selections. They are only the seventh commonest neoplasm in adults (20+ years), yet malignant mind tumors contribute disproportionately to mortality and morbidity in most cancers sufferers. The most common anatomic location of all intracranial tumors is the meninges, followed by the cerebral hemispheres, sellar region, cranial nerves, brainstem, and cerebellum (16-5). Overall, the commonest primary brain tumor in adults is meningioma, adopted by astrocytomas and pituitary neoplasms (16-6). In youngsters age 0-4 years old, the most incessantly reported tumor kind is embryonal neoplasm. The most typical general childhood cancers (ages 0-19 years) are pilocytic astrocytoma and embryonal tumors (two-thirds of that are medulloblastoma) (16-10). Gliomas-second solely to meningiomas in incidence-are one of the heterogeneous group of neoplasms. Glial neoplasms constitute one of the most heterogeneous groups of mind tumors and are the most typical general malignant mind tumor. Tumors of putative glial cell origin had been originally called "gliomas" (because of their supposed derivation from glue-like glial cells). The neuropil accommodates several subtypes of glial cells: astrocytes, oligodendrocytes, ependymal cells, and modified ependymal cells that type the choroid plexus. The commonest total website is the cranial meninges followed by the cerebral hemispheres and sellar area. Meningiomas are the most typical group followed by astrocytomas and pituitary tumors. A paradigm shift in our understanding of most cancers origins has occurred over the earlier couple of years. When these brainstem cells mutate, they turn into tumor progenitor cells (tumor stem cells) that may generate phenotypically various neoplasms. The latter are nosologically extra similar than are diffuse astrocytoma and pilocytic astrocytoma. In time, other pediatric gliomas that seem much like adult neoplasms could also be given separate diagnostic classes. Astrocytomas could be relatively localized (and usually behave extra benignly) or diffusely infiltrating with an inherent tendency to malignant degeneration (16-4). The most typical astrocytomas are diffusely infiltrating neoplasms in which no distinct border between tumor and regular mind is present (even though the tumor may look discrete on imaging studies). Neoplasms, Cysts, and Tumor-Like Lesions 502 (16-7) Graph depicts the relative prevalence of all intracranial tumors in adults. Roughly half are metastases from systemic cancers; the other half are primary neoplasms. The extra localized astrocytic tumors are much less common than the diffusely infiltrating astrocytomas. They are widespread in the cerebellum and around the third ventricle however hardly ever happen in the hemispheres (16-3). Infratentorial ependymomas, typically arising throughout the fourth ventricle, occur predominantly in kids. Supratentorial ependymomas are extra widespread in the cerebral hemispheres than the lateral ventricle and are often tumors of younger children.
Generic coversyl 8mg with mastercard
Adenoid within the operative website: the taste bud is retracted by the pink rubber catheters; adenoid mass (A) is uncovered with the torus tubarius (T) on the lateral side. Operative Risks � E yeinjuries,especiallycornealinjuries,arepreventableby taping the eyes shut with caution. When the pinnacle is draped, watch out not to place the catheters or devices such as towel clips or clamps over the eye space. Bifid uvula, notched exhausting palate, and absence of the muscle of the taste bud (zona pellucida) are signs of submucous cleft palate. Most of the adenoid mass is eliminated by way of the first few swipes utilizing the wide-shaped adenoid curette. Adenoidectomy may be performed as a day surgical procedure in wholesome youngsters not younger than 3 years old with no underlying ailments or suspicious historical past of irregular bleeding. The effect of residual sedative medication after the operation ought to be monitored to avoid respiratory depression. Bleeding is mostly from the raw surface; hemostasis is achieved with electrocautery and adequate nasopharyngeal packing. The techniques and instruments for adenoidectomy had been compared to one another in many studies. Cold curettage was done with less imply operative time however more blood loss when compared to coblation. Rate of revision surgical procedure was not totally different between suction coagulation and cautery in comparability with the microdebrider. Adenoidectomy by suction coagulation supplied much less blood loss when in comparison with a historical control group of adenoidectomy by cold curettage. Complications of adenoidectomy are divided into perioperative and delayed complications. Bleeding from the nasopharyngeal bed is generally uncooked surface bleeding, which is normally stopped by cautery and nasopharyngeal packing with the utilization of a vasoconstrictor. Avoid dissection too deep within the nasopharyngeal mucosa to prevent excessive bleeding. Common Errors in Technique � I njury to the torus tubarius is most likely to occur through the removal of large adenoid pads that obscure the view of the nasopharynx. Rate of revision surgery is roughly in the identical range for all the popular devices: for microdebrider, zero. This could be avoided by a careful history taking and preoperative bodily examination. Physical examination can reveal cleft palate or brief, tight taste bud, or bifid uvula. The pathology is nontraumatic atlanto-axial subluxation due to an inflammation in the prevertebral area. Periligamentous irritation of the anterior transverse ligament causes laxity of the ligament and imbalance of the cervical spine. Nasopharyngeal infection/inflammation and different infections similar to otitis media, tonsillitis, and surgical procedures such as mastoidectomy had been reported to be the trigger of Grisel syndrome, which happens within a week after surgery or infection. The affected person should be evaluated with imaging of the cervical spine and neurosurgical consultation. Treatment contains conservative management with anti-inflammatory drugs, antibiotics, and immobilization. The relationship between the adenoid and pediatric sinusitis was proven by the correlation of micro organism within the center meatus and the adenoid. There was a report of great discount of recurrent sinusitis and obstructive sleep disorder after adenoidectomy. During this period, new instruments and technologies have been launched, but the primary technique of adenoidectomy has remained unchanged. The indications for the procedure, nonetheless, have been revised based mostly on scientific proof.
Purchase 4 mg coversyl visa
Humans-most often children-become accidental intermediate hosts by ingesting eggs in soil contaminated by excrement from a definitive host. Tuberculosis and Fungal, Parasitic, and Other Infections 399 (13-43A) Autopsy case exhibits mind after the removal of an enormous unilocular hydatid cyst. Sometimes a detached germinal membrane and hydatid "sand" can be seen within the dependent portion of the cyst (13-46). Irregular peripheral or ring-like, heterogeneous, nodular, and cauliflower-like patterns have been reported (13-42). Differential Diagnosis the differential diagnosis of a supratentorial intraaxial cystic mass is extensive and contains cystic neoplasms, abscess, parasitic cysts, and neuroglial cysts. Porencephalic cysts are literally "holes in the brain" adjoining to-and normally linked with-an enlarged ventricle. Amebiasis Terminology and Etiology Amebae are free-living organisms which might be distributed worldwide. Species of the Acanthamoeba (Ac) genus are found in soil and dirt, recent or brackish water, and quite so much of different areas starting from sizzling tubs and hydrotherapy swimming pools to air conditioning items, contact lens options, and dental irrigation units. Amebic abscess occurs but is relatively unusual in Western and industrialized countries. Numerous trophozoites are current, however no cysts are seen due to illness acuity. Healthy children and immunocompetent younger adults swimming in heat recent water during the summer are the standard patients, presenting with fever, headache, and altered mental standing. Presentation ranges from headache and chronic low-grade fever to (13-47C) Histology reveals meningitis, hemorrhage/inflammatory cells in Virchow-Robin spaces. Infection, Inflammation, and Demyelinating Diseases 402 (13-51) Sporozoites inoculated into blood infect the liver cells. Merozoites develop into trophozoites or gametocytes, that are then ingested by uninfected mosquitoes. Symptoms are nonspecific and embrace headache, altered psychological status, and meningeal signs. Amebic abscesses and meningoencephalitis can mimic illness caused by different pyogenic, parasitic, and granulomatous infections. The life cycle of a malaria parasite involves the female Anopheles mosquito and a human host. Merozoites can turn into trophozoites, which endure asexual copy within the blood, or into gametocytes, which reproduce sexually in deep tissue capillaries. Gametocytes are ingested by mosquitoes, and the cycle is repeated time and again (13-51). Imaging A broad spectrum of imaging findings in amebic meningoencephalitis has been described, including meningeal exudates, multifocal hemorrhagic parenchymal lesions (1349), and pseudotumoral lesions with necrosis. Multifocal parenchymal lesions with involvement of posterior fossa buildings, diencephalon, and thalamus are typical (13-50). Amebic abscesses are often located in the basal ganglia or on the gray-white matter junction. Solitary or a number of irregularly shaped ring-enhancing hemorrhagic lesions are the typical imaging discovering. Pathology Grossly the brain seems swollen, and its exterior surface is usually a characteristic dusky dark purple. Deposition of malaria Tuberculosis and Fungal, Parasitic, and Other Infections pigment can give the cortex a slate grey colour (13-52). Petechial hemorrhages are sometimes seen within the subcortical white matter, corpus callosum, cerebellum, and brainstem (13-55). Malaria parasites remain intravascular, so encephalitic inflammatory adjustments are absent. Malaria is usually restricted to tropical and subtropical areas with altitudes underneath 1,500 meters and to travelers or immigrants coming from endemic areas. For such circumstances, falciparum malaria occurred in individuals who never traveled outside the country but turned infected by imported anopheline mosquitoes at or round a world airport. Shaking chills followed by cyclical excessive fever and profuse 403 Clinical Issues Epidemiology and Demographics. Falciparum malaria is a number one cause of poor well being, neurodisability, and demise in tropical nations.
Purchase coversyl 8 mg overnight delivery
The thalamus and basal ganglia are the second most typical websites of involvement, adopted by the cerebral hemispheric white matter. Mass effect is often minimal, but, through the acute part, giant brainstem and/or basal ganglia lesions can exhibit significant mass effect, extending into the diencephalon and mimicking neoplasm. Mild to average patchy enhancement following contrast administration is frequent; sturdy, uniform enhancement is uncommon. Skin lesions are generally absent in sarcoid, whereas serum angiotensin-converting enzyme ranges are usually (but not invariably) elevated. Sweet syndrome, also recognized as acute febrile neutrophilic dermatosis, is a multisystem inflammatory disorder that usually manifests as a vasculitis presenting with painful erythematous skin plaques, fever, and leukocytosis. Most diagnoses of lupus are established on the idea of systemic findings and laboratory abnormalities with imaging enjoying an essential but ancillary position in diagnosis and management. Multiple parts of the immune system are affected, together with the complement system, T suppressor cells, and cytokine merchandise. Vasculopathy Activation of the complement system, along with formation and deposition of immune complexes in tissues, recruits B lymphocytes, resulting in formation of autoantibodies. Immune system dysfunction additionally leads to frequent infections and increased prevalence of lymphoreticular malignancy. Lupus-related cerebral ischemia/infarction may result from coagulopathy (secondary to antiphospholipid syndrome), accelerated atherosclerosis (often related to corticosteroid treatment), thromboembolism (secondary to Libman-Sacks endocarditis), or a real main lupus vasculitis. Lupus angiitis/vasculitis is characterized histopathologically by marked endothelial hyperplasia and obliterative intimal fibrosis in small arteries and arterioles. Occlusive fibrin thrombi with out histologic proof of vasculitis can also happen. Diffuse cortical, basal ganglia, and brainstem lesions-suggestive of vasculopathy or vasculitis-are additionally widespread. Acute lesions show transient enhancement on T1 C+ research and restricted diffusion. The spectrum of antiphospholipid-mediated syndromes displays end-organ damage because of microangiopathic disease and endothelial dysfunction. Nontraumatic Hemorrhage and Vascular Lesions 316 accelerated and widespread vessel occlusions and has a mortality rate approaching 50%. Two amino acid species, a 42-aa length (A42) and a shorter 40-aa (A40) size, are associated with amyloid-related mind disease. These deposits accumulate within the abluminal portion of the muscular layer and adventitia of cerebral arterioles and capillaries, causing progressive disruption of the neurovascular unit. The geographic distribution of A deposits corresponds anatomically to the perivascular drainage pathways by which interstitial fluid and solutes are eradicated from the mind. Gross pathologic findings include major lobar hemorrhages (most commonly frontal or frontoparietal), cortical petechial hemorrhages, small cerebral infarcts, and white matter ischemic lesions (10-65). Microscopic features embody a "smudgy" eosinophilic thickening of leptomeningeal and cortical vessels (10-66). Severe cases can show vessel "splitting" (a "lumen within a lumen" appearance), fibrinoid necrosis, pseudoaneurysm formation, and thrombosis. A-related angiitis demonstrates mural and perivascular inflammatory adjustments with necrosis, variable numbers of multinucleated giant cells, epithelioid histiocytes, eosinophils, and lymphocytes. A attribute yellow-green shade ("birefringence") appears when the affected vessels are considered utilizing polarized gentle (10-67). Amyloidladen blood vessels are additionally immunoreactive for matrix metalloproteinase19. Multiple irregular confluent white matter hypointensities along with generalized quantity loss are widespread. Vasculopathy Shiga toxins cause widespread vascular endothelial harm that in flip leads to multiorgan infarcts and hemorrhages. Arteriolar and capillary wall thickening, endothelial swelling and fragmentation, subendothelial accumulation of protein and cellular particles, and a quantity of platelet-fibrin occlusive thrombi are attribute histopathologic findings (10-72). Fever, renal insufficiency, and a purpuric rash over the trunk and limbs are common.
Order online coversyl
An example of "open framework" on the right (Jabbour); antihelix is augmented with items of cartilage sutured to the primary framework. Typical examples of postoperative view instantly following stage I reconstruction (left) and 1-week postoperative (right). The movie then could also be minimize to develop a template that may be sterilized for use in the first stage of surgery. Patients must be counseled on the importance of postoperative care and advised on sensible surgical outcomes. Positioning Supine: the patient is positioned supine so that each ears may be seen and accessed during the process. Perioperative Antibiotic Prophylaxis First-generation cephalosporin Second-generation cephalosporin Clindamycin if allergic to penicillin. A pocket is created in the lobule to insert the inferior aspect of the cartilage framework. Excess pores and skin on the superior side of the lobule is used to deepen the conchal bowl, and a quantity of smaller W-plasty incisions are performed to irregularize the scar. Suture: 4-0 undyed nylon suture, 3-0 and 4-0 Vicryl suture, 5-0 monocryl suture, or comparable 4. Scarring Preoperative Preparation � Design of auricular template from flipped image of contralateral auricle (if available). This may be performed by printing a horizontally-flipped picture in photo enhancing software or by tracing the contralateral ear with transparency film. Rectus abdominus-inserts to cartilaginous parts of fifth, sixth, and seventh ribs and xyphoid process. External abdominal indirect muscles-origin is exterior surfaces of ribs 5 to 12; inserts to abdominal aponeurosis. Internal stomach indirect muscles-has insertions into ribs eight to 12 and stomach aponeurosis. Intercostal space-Neurovascular bundle runs within the superior aspect of each intercostal space within the order of vein, artery, nerve, from superior to inferior. Costochondral junction-The bony to cartilaginous junction of each rib can be identified by the modifications in color on the junction and confirmed with a 25-gage needle intraoperatively after exposing the rib, as the needle will pass extra simply into the cartilaginous portion. Surgical Technique There are two techniques: (1) three-stage Bonilla method and (2) four-stage approach. Stage I-Creation and Insertion of Cartilage Framework and Tragus � Preoperative � Mark patient ear and rib to affirm laterality in preoperative area. Have the nose uncovered, as the angle of the nasal dorsum parallels the best auricular angle. Skill and experience in carving costochondral cartilage for microtia reconstruction 3. The framework is elevated and a polyethylene implant wedge is placed for projection and is roofed with a conchal-based flap and full-thickness pores and skin graft. A small layer of cartilage is left covering the junction to avoid a hard, pointed remnant of the bony rib. The timing of this placement is variable; if placed prior to rib harvest, decreased narcotic use through the case could also be possible; if positioned in the course of the cartilage carving, decreased operative time may be achieved. The helical crus is then formed by excising probably the most medial portion of the eighth rib cartilage to make a barely pointed edge. In order to cause a bend of the cartilage, the outer edge is trimmed and the perichondrium is removed very fastidiously with a scalpel. The x-ray template is then positioned over the synchondrosis in order to measurement the model new ear. If the synchondrosis cartilage is too thick, it might be thinned by trimming with a scalpel. If the pores and skin pocket is too thin, there might be a threat of ischemia and potential necrosis of the skin with subsequent publicity of cartilage. Microtia 1473 � Antibiotic ointment is placed over the incision web site and the drain website, and a telfa dressing is then utilized over the ear. Care ought to be taken to ensure that the wedge implant is absolutely coated previous to skin grafting.
Purchase coversyl pills in toronto
The lateral crural overlay is depicted right here with the purple areas displaying the realm of overlap. A vertical dome division is carried out with a cephalic trim and reconstructed with interdomal sutures and reapproximating the lateral crura to the tip cartilages. By combining the overlapping technique of the medial and lateral crura, the surgeon can exercise control over each the diploma of rotation and projection simultaneously. Care have to be taken to not excessively destabilize the tip with extra intensive maneuvers. Lateralcrural struts can be utilized to improve a boxy nasal tip, malpositioned or extreme cephalic lateral crura, rim retraction, and concave lateral crura. These present less thickness to the septal cartilage in the space of overlap of the septal extension graft with the septum but additionally lack the stability that this overlap provides. The nasopharynx is suctioned, and an orogastric tube is handed to decompress the abdomen and esophagus prior to reversal of anesthesia. These are handled with secondary rhinoplasty to handle the particular explanation for the bossae. This is controversial due to reviews of vascular complications (embolization of filler material) however is an increasingly widespread procedure. This is began the day of surgical procedure and continued whereas the splints stay in place. Evidence-Based Medicine Question Do goal measurements of nasal proportions correlate with facial attractiveness A research of 300 lateral facial views confirmed no correlation amongst these measurements (as described by Goode, Simons Baum, Powell, and Crumley) with each other or with facial attractiveness as assessed by 78 viewers. This is just one of many illustrations that should make readers skeptical about counting on any single goal measurement too much with out assessing the patient as an entire. Complications � P olybeak deformity-appears as dorsal fullness and may result from over-resection of the nasal bones, under-resection of the cartilaginous septum, or scarring of the supratip region and is treated with steroid injection within the case of scarring or secondary rhinoplasty to tackle the anatomic trigger � O pen roof deformity-manifests as a widened and incessantly asymmetric bony nasal dorsum. Lateral crural steal (recruitment of lateral crural cartilage to the midline) would have which effect on tip rotation and nasal projection Size, shape, configuration, and symmetry of the bony orbit and palpebral aperture. Brow position: Determine the extent to which brow ptosis could be contributing to the obvious upper eyelid skin extra. In males, a youthful brow place rests on the degree of the superior orbital rim; in ladies, best forehead position is about 1 cm above the orbital rim. Significant forehead ptosis should immediate a dialog with the affected person concerning the merits of a brow-lift or combination brow-lift and blepharoplasty. Eye closure: Pre-existing lagophthalmos is an absolute contraindication to higher eyelid blepharoplasty. Depending on the experience of the surgeon, ptosis repair would possibly require the expertise of an oculoplastic surgeon. Record the degree of extra skin in every eyelid and adipose tissue in each adipose tissue compartment (medial and central compartments). Consider different methods to standard skin-muscle decrease lid blepharoplasty or a concomitant canthoplasty or canthopexy. In addition, observe how lengthy it takes for the decrease lid to return to its pretest position. Record the degree of excess pores and skin in each eyelid and adipose tissue in every adipose tissue compartment (medial, central, and lateral compartments). Excess adipose tissue in the lower lid compartments is accentuated by upward gaze. The periorbital region is among the first areas of the face to present signs of growing older. Correction of this imperfection can considerably "flip again the clock" of growing older and has thus led to the popularity of aesthetic surgery on the eyelids. Owing to the important position that the upper and lower eyelids serve in protecting the globe, the surgeon have to be very attentive to the delicate stability between form and performance when performing blepharoplasty.
Discount coversyl 8mg without prescription
Which reconstructive technique delivers probably the most predictable reconstructive end result in remedy of full-thickness scalp defects with cranial publicity Drilling out of the cranium outer table and adverse stress wound remedy adopted by skin graft b. Effect of advanced age and medical disease on the end result of microvascular reconstruction for head and neck defects. Practitioners in historic India were the primary identified to harvest pores and skin from the forehead to repair facial defects, primarily of the nose. Due to nasal amputation as a common form of judicial and political punishment on the time, there was ample opportunity for the practice of reconstruction using forehead skin. Interestingly, the practitioners of the brow flap surgical process belonged to the potter and tilemaker castes somewhat than that of the physicians. This method was stored as a closely guarded secret, passed down through oral tradition. Further exploration and refinement of the brow flap as a way of reconstruction followed throughout the 20th century. Forehead tissue is currently the gold standard for nasal reconstruction and is also used for lots of different facial defects. This article examines the utilization of the forehead flap in repairing defects of the pinnacle and neck. If a affected person is taking anticoagulation medicine, the need of the anticoagulation and the potential well being dangers of momentary cessation or bridging should be weighed. Forexb S ample, the three-dimensional contour of a large nasal defect requires precise planning. To avoid the hairline, the flap can be lengthened by extending the incisions inferiorly into the forehead or by designing it barely obliquely. The mechanism of tissue loss may be excision of a cancer, trauma, infection, or congenital defects. A, Tissue enlargement full, template of the nasal defect outlined on the expanded brow flap. Preoperative Preparation � T here are many choices for the reconstruction of nasal defects. The surgeon and the affected person ought to carefully determine which best fits the needs of the defect and the affected person. Healing by secondary intention, major closure, skin grafting, and different native flaps are different choices (see Chapter 163). The distance from the bottom of the brow flap to the defect should be meticulously measured to ensure adequate length once the flap is rotated. General anesthesia is preferable for many brow flaps for affected person consolation and intraoperative planning. Either lidocaine or a combination of lidocaine and bupivacaine will work nicely for local anesthetic infiltration, and benzodiazepines given intravenously might present adequate leisure and sedation. The terminal department is the angular artery, which supplies off the lateral nasal department before persevering with a superomedial course past the medial canthus to anastomose with the dorsal nasal artery and infrequently withthesupratrochlearartery. Afterthisanastomosis, the angular artery contributes to a central artery, which courses in a superior course near the midline of the forehead. The parietal branch supplies the posterosuperior scalp, and the frontal department programs anteriorly to provide the lateral brow where it anastomoses with the supraorbital artery. Instruments and Equipment to Have Available � P lastic surgical procedure soft tissue tray containing #15 C blades, small double-pronged skin hooks, iris scissors, and zero. However, landmarks could reliably be used to locate the supratrochlear artery as an alternative of a Doppler. One can then examine to see if the flap size and design are appropriate for the defect. Thedonorsitemaybequite conspicuous when a large laterally based flap is used for midface defects. If the pedicle is twisted, causing decreased perfusion, it could be indifferent from the defect and rotated back into its native position to reestablish blood circulate.
Order coversyl 4mg with visa
Biologic conduct is variable, and long-term survival-even with subtotal resection-is widespread. Papillary tumor of the pineal area can seem identical on imaging studies but may be very rare. A soft, friable, diffusely infiltrating tumor that invades adjoining mind and obstructs the cerebral aqueduct is typical (20-13). Occasional Homer-Wright rosettes (neuroblastic differentiation) or Flexner-Wintersteiner rosettes (retinoblastic differentiation) can be identified (20-15). Clinical Issues (20-14) Autopsied pineoblastoma shows dissemination with metastases coating lateral, third ventricles. Symptoms of elevated intracranial stress similar to headache, nausea, and vomiting are typical. Surgical debulking with adjuvant chemotherapy and craniospinal radiation comprise the everyday routine. A massive, hyperdense, inhomogeneously enhancing mass with obstructive hydrocephalus is typical. If pineal calcifications are current, they appear "exploded" towards the periphery of the tumor (20-16A). Pineal anlage tumors are a peculiar, very rare malignant pineal tumor of infants and young youngsters. No endodermal elements are present, distinguishing these uncommon tumors from teratomas. Imaging exhibits a combined solid and cystic pineal area mass that typically causes obstructive hydrocephalus. Progression-free survival in sufferers with a low frequency of hypermethylated genes is almost 3 times longer than these with larger methylation ranges (125 months vs. No options that may distinguish these tumors from pineal parenchymal tumors of intermediate (20-20) the patient deteriorated 5 weeks later. Pineal and Germ Cell Tumors 619 (20-21) Autopsy of a posterior third ventricular mass that invades midbrain tegmentum reveals cysts, hemorrhage. They differ in malignancy from mature teratomas to poorly differentiated, extremely aggressive neoplasms similar to embryonal carcinoma, choriocarcinoma, and endodermal sinus (yolk sac) tumors. Intracranial germinomas have a definite predilection for midline structures (20-23). Between 80-90% "hug" the midline, extending alongside the midline axis from the pineal gland to the suprasellar area. One-half to two-thirds are found in the pineal area with the suprasellar region the second most frequent location, accounting for one-quarter to one-third of germinomas. Note severe obstructive hydrocephalus with "halo" of fluid round each temporal horns. Neoplasms, Cysts, and Tumor-Like Lesions 622 Nongerminomatous subtypes predominate at other websites. The most frequent combination is a pineal plus a suprasellar ("bifocal" or "double midline") germinoma (20-24). Germinomas are usually solid, friable, tanwhite plenty that often infiltrate adjoining buildings. Germinomas are histologically similar to ovarian dysgerminoma and testicular seminoma. A pure germinoma consists of huge, comparatively undifferentiated cells with distinguished nucleoli organized in monomorphous sheets or lobules separated by nice fibrovascular septa. Nearly all germinomas have a biphasic sample of abundant reactive lymphocytes-usually dominated by T cells-intermixed with massive round germinoma cells with outstanding nucleoli (20-25). Some tumors exhibit such a florid lymphoplasmacellular reaction that it could obscure the neoplastic components. Occasionally germinomas provoke an intense granulomatous response that mimics sarcoidosis or tuberculosis.