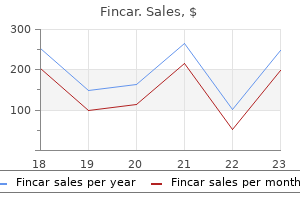
Fincar dosages: 5 mg
Fincar packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

Buy fincar 5mg on line
Objects identified by color among numerous distracters may be situated almost instantly in visual search and shade is invaluable in perceptual grouping and segmenting objects. With regard to mechanism, colour imaginative and prescient is based on three kinds of cone photoreceptors that are the idea for all vision excluding imaginative and prescient beneath very dim light conditions, which is dependent on rods. Perception of black, white, and grey, the hues of red, green, blue, and yellow and their patterns within the retinal picture are extracted by various kinds of ganglion cells each specialised to carry specific information about the visible stimulus from one mosaic of cones. The first limb of the curve displays recovery of cones, and the second, slower limb reflects rod restoration. In this diagram the cones are coloured blue, green, or red to have the ability to represent the different photoreceptor classes. Midget ganglion cells have heart surroundreceptive fields with the middle derived from a single cone (for instance, within the internal ring of the two black concentric circles). The six adjacent cones are crucial contributors to the encompass (for example, the cones inside the outer ring of the 2 black concentric circles). In a traditional trichromat the surrounds of many L or M cones will have some cones of a special kind than the center. In a dichromat, normally all the cones in the encompass are of the same class as the center input to a midget ganglion cell. Clues toward solving the puzzle come from information about the evolution and improvement of visible system and about its anatomy and physiology. In contrast to our persisting ignorance about shade imaginative and prescient circuitry, the last 20 years has seen an explosion of details about the cone photopigments. Many of the long standing questions about these pigments and their function in normal vision and vision issues have now been answered. In humans there are three types of cone photopigment, one for each class of cone (see Box 123. The L and M cone opsins and the genes that encode them are unusually variable, presumably as a outcome of the unstable tandem association of the genes and their unique evolutionary history. Strong selective strain favoring trichromatic color imaginative and prescient acted on primates within the wild, minimizing the prevalence of mutant L and M opsin gene arrays despite the intense instability inherent in tandemly duplicated genes. However, in humans, choice in opposition to mutant X-linked pigment genes has been relaxed. The variability that has resulted consists of gene arrangements responsible for colour blindness, which is the most typical of all human single locus genetic disorders. The increasing proportion of mutant cone pigment genes can be presumably the root of a growing variety of different issues and complications of human imaginative and prescient. Compared to many different widespread inherited recessive issues, similar to cystic fibrosis and sickle cell anemia, colour imaginative and prescient deficiency is uncommon in occurring at an exceptionally excessive frequency with no compelling evidence of a powerful heterozygote benefit to explain why. For example, cystic fibrosis is the most-common life-limiting autosomal recessive disorder amongst humans, estimated to happen at a fee of about one in 3200 live births. Another instance is sickle cell anemia by which heterozygotes are protected in opposition to the extreme pathogenesis of malaria. Genetic evidence indicates that all vertebrate opsin genes evolved from a common ancestor through a process of gene divergence and duplication. In New World primates, trichromatic shade vision was acquired via evolution of allelic range within the X-chromosome opsin gene, which produced variety in spectral sensitivity of the encoded photopigments. In Old World primates, trichromatic shade imaginative and prescient arose via a gene duplication that positioned two opsin genes together in tandem on the X-chromosome. Calling them short-, middle-, and long-wavelength sensitive, abbreviated S, M, and L cones minimizes confusion that can arise from giving them color names. Photopigment molecules within every cone are responsible for the spectral properties of the cones. Each photopigment molecule consists of two components; a protein termed the opsin, and an 11-cis-retinal chromophore. The noncontributing cone class is indicated by the prefixes: Protan- for absence of L cone contribution to vision. Further categorization of shade vision defects is determined by whether or not the remaining color imaginative and prescient is based on two (dichromacy) versus three (anomalous trichromacy) spectrally distinct forms of cones.
Diseases
- Thanatophoric dysplasia Glasgow variant
- Neurasthenia
- Klumpke paralysis
- Oculo cerebro osseous syndrome
- Toxoplasmosis
- Von Hippel Lindau disease
- Familial multiple trichodiscomas
- Arthrogryposis ectodermal dysplasia other anomalies
Fincar 5 mg otc
Reduction of intraocular stress through ocular antihypertensives and paracentesis which theoretically can also dislodge an embolus have been attempted to enhance retinal arterial circulation. Studies have shown no significant difference in ultimate versus preliminary visual outcomes in use of topical beta blockers, oral acetazolamide, or paracentesis. While results of one study discovered that the pentoxifylline group had much less neovascularization in comparability with standard therapy, there was no definitive improvement in visible outcomes. This modality of treatment has not shown benefit to ultimate visible end result and is usually now not used. Laser picture disruption of an embolus has been reported in select sufferers to trigger passage of the embolus via the arterial tree with improvement in outcomes. The second side of management of retinal arterial occlusive disease is systemic workup. Panretinal laser photocoagulation may be efficacious in preventing the development of neovascular glaucoma. Focal laser photocoagulation in ocular ischemic syndrome patients with macular edema is another therapy modality the place efficacy has not been confirmed through randomized managed medical trials, however may be affordable. Prompt referral to an internist, neurologist, or vascular surgeon is necessary to handle modifiable risk components and to contemplate carotid endarterectomy within the applicable patient. The efficacy of endarterectomy in stroke prevention in symptomatic sufferers with 70�99% stenosis has been demonstrated in the North American symptomatic carotid endarterectomy trial. In as a lot as 30% of patients, no systemic associated condition leading to arterial occlusion is documented. The most devastating long-term ocular complication of retinal arterial occlusive illness is neovascular glaucoma. While the eye sometimes has restricted vision secondary to the initial occlusion, the choice of a restricted vision, comfy, cosmetically acceptable eye versus a blind painful eye is apparent. Treatment is as with any different type of neovascular glaucoma with laser or cryotherapy to the retina and ciliary physique and topical antihypertensive medications. The ocular ischemic syndrome can be outlined as a syndrome of hypoperfusion to the globe secondary to carotid artery or more not often ophthalmic artery occlusive illness. Patients with the ocular ischemic syndrome may be asymptomatic initially or could notice gradual blurring, typically of a transient nature. Patients are typically 50 years old or older and infrequently have significant atherosclerotic illness with other cardiovascular or cerebral vascular symptoms. Posterior section findings embrace retinal hemorrhages in all 4 quadrants, sometimes present in the midzone. This is a differentiating characteristic from central retinal vein occlusion the place veins are dilated. Microaneurysms and macular edema could additionally be current and in advanced instances neovascularization of the disk or retina could also be present. It is important to make the analysis of ocular ischemic syndrome as a end result of these sufferers usually develop cerebral vascular accidents. Fluorescein angiogram shows delayed filling of retinal arterials with asymmetric filling of the choroid. Progressive arterial filling with delayed venous filling and extended venous transit time and continued asymmetric filling of the choroid. Leakage from neovascularization of the disk with late staining of the retinal vessels. Ozdemir H, Karacorlu S, Karacorlu M, et al: Optical coherence tomography findings in central retinal artery occlusion. Ashton N, et al: Focal retinal ischemia, ophthalmoscopic, circulatory and ultrastructural adjustments. Kramer M, Goldenberg-Cohen N, Shapira Y, et al: Role of transesophageal echocardiography within the evaluation of sufferers with retinal artery occlusion. Greiner K, Hafner G, Dick B, et al: Retinal vascular occlusion and deficiencies within the protein C pathway. Pianka P, Almog Y, Man O, et al: Hyperhomocystinemia in patients with nonarteritic anterior ischemic optic neuropathy, central retinal artery occlusion, and central retinal vein occlusion. Dori D, Beiran I, Gelfand Y, et al: Multiple retinal arteriolar occlusions related to coexisting main antiphospholipid syndrome and factor V Leiden mutation.
Order fincar with a mastercard
Since the Nineteen Seventies, the pattern has shifted from intracapsular to extracapsular surgery. Concurrent with the development towards the outpatient setting has been a pattern toward the usage of fewer preoperative sedative drugs, with a shorter duration of motion. In 1995, it was reported in a survey of 1500 ophthalmologists in the United States that 50% used retrobulbar injection, 38% used peribulbar injection, 11% used topical anesthetic or topical anesthetic supplemented with a subconjunctival injection, and zero. Some surgical issues which may be prevented by operating on a gentle eye include anterior displacement of the lens�iris diaphragm, causing shallowing of the anterior chamber; lack of vitreous; and expulsive choroidal hemorrhage. Various preoperative methods embrace the appliance of digital or other means of exterior strain to the globe. Topical mydriatics are usually instilled preoperatively, and many surgeons additionally use an intracameral mydriatic intraoperatively to preserve pupillary dilatation. A variety of agents can be found, including adrenergics, anticholinergics, and prostaglandin inhibitors. They are mostly administered for diagnostic ophthalmoscopy, refractions, provocative checks for angleclosure glaucoma, or the therapy of anterior uveitis and secondary glaucomas. One methodology of conjunctival preparation generally practiced is the instillation of 1 or two drops of a 5% iodine answer applied to the conjunctival cul-de-sac. This has been proven to considerably scale back the bacterial depend and the variety of species current on the ocular surface. Some surgeons also prescribe a broad-spectrum preoperative topical antibiotic that covers a lot of the widespread organisms of ocular floor flora. During extracapsular cataract surgery, exposure of the superior limbus is important. To achieve this downward rotation of the attention, most extracapsular surgeons use a superior rectus traction suture. The placement of a traction suture may help in lifting a deeply set globe from the orbit. Some surgeons really feel that this method is related to postoperative ptosis, although this has been debated. The globe is then rotated inferiorly as the fixation suture is mounted to the drape. The flap is folded and pulled in a circular movement so that the pressure at the point of the tear is tangential to the circumference of the circle. The incision is created parallel to limbus and apart 2�3 mm posterior to the limbus. The incision should be created perpendicular to the scleral surface and to ~70% depth of the total scleral thickness. Then, ~4 mm of scleral/corneal dissection ought to lengthen to the anterior chamber entry position. A lens loop is often used superiorly, and one other blunt instrument, corresponding to a forceps or a muscle hook is used inferiorly. As stress against the globe is alternated between the two instruments, the nucleus begins to move by way of the incision at the superior limbus. Another variation involves removing of the nucleus directly from the posterior chamber using a vectis. Injecting viscoelastic material will act as a cushion from the nucleus to prevent corneal endothelial cell injury. After the nucleus has been removed, the irrigation�aspiration handpiece is handed between the sutures into the anterior chamber. This course of is continued until the cortex is completely eliminated and the capsular bag is obvious. If the posterior capsule inadvertently becomes engaged into the aspiration port, aspiration have to be rapidly disengaged and the reflex system employed. This is finished by hand and with both a reflex bulb or a foot pedal mechanism in automated devices. The lens now could also be rotated barely so that the haptics are positioned horizontally and the optic is properly centered.
Purchase discount fincar online
Surgical techniques include some combination of cryotherapy of the concerned cornea with the anterior chamber filled with Postoperative opacification of initially clear posterior capsules happens frequently in patients after cataract surgical procedure, although the time to opacification is very variable. In adults, the time from surgery to visually important opacification varies from months to years,one hundred twenty five and the speed of opacification declines with increasing age. Mitotic inhibitors instilled into the anterior chamber after extracapsular cataract extraction has been proven to cut back capsular opacification dramatically. Fibrosis connotes a gray-white band or plaque-like opacity which may be recognized within the early postoperative period or could happen later. Fibrosis that develops months to years postoperatively is caused by migration of anterior lens epithelium, fibroblastic metaplasia, and collagen production. The fibrosis is clear with indirect slit-lamp illumination (a) but is optically insignificant when viewed with a red reflex (b). Topical apraclonidine and brimonidine have been shown to be highly efficient in stopping acute pressure spikes following laser treatment. Dense fibrosis on the edge of a posterior chamber intraocular lens optic positioned in the bag (arrow) by which an anterior capsular flap is apposed to the posterior capsule. This syndrome has been reported to happen with small capsulorrhexis openings of less than 6 mm. Acrylic lenses have the bottom charges whereas silicone plate lenses appear to have the highest rates. This sort of opacity occurs from proliferating lens epithelial cells, which might form layers of a quantity of cells thick. Broad undulations of clear capsule are significantly common in the early postoperative period before the capsule turns into tense. Posterior chamber lens haptics could induce these broad wrinkles alongside the axis of the hepatic orientation. Conversely, a posterior chamber lens might tend to flatten broad wrinkles if the optic physique presses on the capsule. Broad, undulating wrinkles of clear capsule not often are visually disturbing to the patient; an uncommon affected person may perceive linear distortion or shadows that correspond to the wrinkles, that are relieved by capsulotomy. In distinction, fine wrinkles or folds in the capsule, caused by myoblastic differentiation, may find yourself in marked optical disturbance. These fine wrinkles are brought on by myofibroblastic differentiation on the migrating lens epithelial cells, which acquire contractile properties, resulting in the wrinkles. The diplopia is most commonly due to inferior rectus muscle restriction but has been reported within the superior and lateral recti muscle tissue. Without the addition of hyaluronidase, the speed of muscle restriction has been discovered to be significantly increased. Intolerable unwanted optical photographs constitute another legitimate purpose for explantation. Suturing a posterior chamber lens via either the iris or the ciliary sulcus presents a further method for lens trade, especially in a patient with glaucoma or with an abnormal anterior phase. The course of action must replicate the kind and site of the lens, the age of the affected person, the symptoms, the visible acuity, the corneal endothelial well being, the presence and severity of intraocular inflammation, and the status of the fellow eye. When surgical intervention is under consideration, a call should be made with regard to the timing of surgery, the strategy (anterior versus posterior), the composition of the surgical group (cataract surgeon, vitreal surgeon, or both), and the disposition of the pseudophakes (repositioning, substitute, or removal). Edge-related reflections, diplopia, or glare might in some cases be managed efficiently by topical pilocarpine in weak concentrations similar to zero. Topical sodium chloride could be preferable to surgery in treating peripheral corneal edema related to incipient corneal decompensation in an aged patient who has a low endothelial cell rely. The commonest presenting criticism is unwanted optical pictures brought on by either a positioning hole or the edge of the optic throughout the pupil. If the symptoms are rare and restricted to evening when the pupil is more dilated, the surgeon might elect to manage these patients conservatively through the use of a topical miotic. The introduction of suturing strategies both for secondary placement of posterior chamber lenses and for repositioning of dislocated lenses has further elevated the obtainable choices.
Carex arenaria (German Sarsaparilla). Fincar.
- Preventing gout, inducing sweating, arthritis, skin problems, fluid retention, sexually transmitted diseases (STD,VD), intestinal gas, colic, liver problems, diabetes, tuberculosis, lack of menstruation (periods), and other conditions.
- Dosing considerations for German Sarsaparilla.
- Are there safety concerns?
- What is German Sarsaparilla?
- How does German Sarsaparilla work?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96467
Generic fincar 5mg
Intravitreal injection of triamcinolone: an emerging treatment for diabetic macular edema. Glucocorticoid regulation of endothelial cell tight junction gene expression: novel therapies for diabetic retinopathy. An ocular clinicopathologic correlative examine of six sufferers from the Diabetic Retinopathy Study. Characterization of macular edema from varied etiologies by optical coherence tomography. The exudative lesions in diabetic retinopathy with special regard to the onerous exudate. Tractional cystoid macular edema: a refined variant of the vitreomacular traction syndrome. Optical coherence tomography assessment of the vitreoretinal relationship in diabetic macular edema. Impaired color imaginative and prescient related to diabetic retinopathy: Early Treatment Diabetic Retinopathy Study Report No. Temporal variation in diabetic macular edema measured by optical coherence tomography. Diurnal variation in retinal thickening measurement by optical coherence tomography in center-involved diabetic macular edema. Ophthalmoscopy versus photography- Early Treatment Diabetic Retinopathy Study Report Number 5. Reproducibility of macular thickness and volume utilizing Zeiss optical coherence tomography in patients with diabetic macular edema. Repeatability and reproducibility of quick macular thickness mapping with stratus optical coherence tomography. Errors in retinal thickness measurements obtained by optical coherence tomography. Detection of diabetic foveal edema: contact lens biomicroscopy compared with optical coherence tomography. Comparison of the clinical prognosis of diabetic macular edema with diagnosis by optical coherence tomography. Diabetic macular edema assessed with optical coherence tomography and stereo fundus photography. Comparison of the modified Early Treatment Diabetic Retinopathy and delicate macuilar grid laser methods for diabetic macular edema. The correlation between fluorescein angiographic and optical coherence tomographic options in clinically significant diabetic macular edema. Intravitreal triamcinolone acetonide for diabetic diffuse macular edema: preliminary outcomes of a prospective controlled trial. Oscillatory potentials, macular recovery time, and diabetic retinopathy through three years of intensified insulin treatment. Multifocal electroretinogram and shortwavelength automated perimetry measures in diabetic eyes with little or no retinopathy. Retinal function in normal and diabetic eyes mapped with the sluggish flash multifocal electroretinogram. Visual fields correlate higher than visible acuity to severity of diabetic retinopathy. Visual acuity and perimetry as measures of visible function in diabetic macular oedema. The use of scanning laser ophthalmoscope microperimetry to detect visible impairment attributable to macular photocoagulation. Vitrectomy for diabetic macular traction and edema related to posterior hyaloidal traction. Modified grid laser photocoagulation versus pars plana vitrectomy with inside limiting membrane removal in diabetic macular edema. Vitrectomy leads to diabetic macular oedema without evident vitreomacular traction. Prospective analysis of intravitreal triamcinolone acetonide injection in macular edema associated with retinal vascular issues. Time course of adjustments in retinal thickness and visible acuity after intravitreal triamcinolone acetonide for diffuse diabetic macular edema with and with out previous macular laser remedy.
Generic fincar 5mg line
The recovery of sensitivity in the dark after prior publicity to a bright stimulus is identified as dark adaptation. The speed with which a brand new equilibrium is reached is dependent upon the path and magnitude of the change. In common, discount in sensitivity occurs rapidly relative to restoration of sensitivity. That is, it takes a matter of seconds to adapt to a brighter background, whereas adjustment to decreases in background intensity is slower. After exposure to a brilliant stimulus, the exact time needed to regulate to a dimmer background is dependent upon whether rods or cones are being examined and on the depth of the prior publicity. In the extreme situation, in which one is plunged from a really bright surroundings into full darkness, it can take as much as an hour for rod sensitivity to recuperate totally. Measuring the dark-adaptation curve is the usual methodology for tracking this restoration course of. One plots the threshold as a operate of time after the termination of the conditioning mild stimulus. The shape of the dark-adaptation curve is dependent upon the check stimulus parameters, corresponding to dimension, shade, and retinal location, in addition to conditioning stimulus parameters, similar to its intensity, length, and colour. Fortunately, to an excellent degree these a quantity of components can be reduced to simply two principal figuring out variables. These are the extent to which the take a look at mild stimulates rods and cones and the quantity of visual pigment that has been bleached by the exposure to the conditioning stimulus (see Box 123. If the dimensions, shade, and retinal location are organized so that the check flash stimulates both rods and cones, and significant quantities of rod and cone pigment are bleached by the conditioning stimulus, then dark adaptation proceeds in two distinct phases. In the first phase or department, sometimes lasting ~5�10 min, the threshold is set by the cones as they recover their sensitivity. Later, the rods get well sufficiently for his or her thresholds to be lower than these of the cones, they usually mediate threshold, giving rise to a rod department in the curve. Complete restoration of rod sensitivity takes as lengthy as it takes for rod pigment to regenerate. Few of us would accept a black and white tv or monochrome computer monitor instead of shade ones even in exchange for big financial savings in price. One purpose shade is important to us is that it has a robust effect on our feelings. This is presumably, in part, as a result of some parts of our shade imaginative and prescient system are evolutionarily ancient, predating other sensory capacities. Color can sign the presence of an damage or illness, the presence and or quality of food, and the identification of a mate. In our fashionable world color-coding is extraordinarily necessary in transmitting data visually. The suffix -anomaly denotes anomalous trichromacy in which two of the cone classes are more comparable in spectral sensitivity than the corresponding regular cones: Deuteranopia. The variety of normal and faulty colour vision phenotypes in people is produced by unequal homologous recombination during meiotic cell division in females. The shade of the arrowhead signifies whether or not the gene encodes an L pigment (red) or M pigment (green). Only the two 5, genes (left-most) within the three gene array are expressed and each of those encode L-class pigments. The array produces dichromatic colour imaginative and prescient if the encoded L-class pigments have equivalent spectral properties, or it produces anomalous trichromacy if the pigments differ in spectral properties. The different recombinant array contains a single gene, which encodes an L opsin and thus produces dichromatic color vision. As will be discussed under, the variety launched by intermixing L and M opsin gene sequences underlies the number of phenotypes associated with anomalous trichromacies. Only among humans is there widespread variability within the number of visual pigment genes on the X-chromosome with a excessive frequency of arrays containing greater than two opsin genes. The degree to which colour imaginative and prescient is impaired is decided by the spectral properties of the pigments encoded by the genes that remain.
Generic 5 mg fincar overnight delivery
At later levels, visible problems might embody macular edema, vitreous hemorrhage from neovascularization, epiretinal membrane, or retinal detachment. Approximately 50�60% of untreated sufferers will have a last visual acuity of 20/40 or higher. With time, the fundus findings may turn into much less distinct and seem just like what one would anticipate to see in diabetic retinopathy, hypertensive retinopathy, or different systemic illnesses inflicting retinal microaneurysms and hemorrhages. In nonperfused instances, sclerosis and sheathing of the retinal veins and arteries in the distribution of the occlusion may be noticed. Angiographic findings mirror changes in vessel permeability, caliber, and patency and assist in identifying areas of macular edema, neovascularization, and nonperfusion. Occasionally, early hyperfluorescence simply proximal to the site of occlusion is observed. Macular edema often takes on a petalloid pattern typical of cystoid macular edema. When evaluating for macular edema, it is important to observe whether or not capillary perfusion is current. Neovascularization of the retina or disk appear as early hyperfluorescent, skinny, tortuous vessels that leak within the later stages of testing. Collateral vessels may develop between an space of nonperfused and an space of perfused retina. Although the world of affected retina is small, the hemorrhage and edema lengthen into the fovea and are related to decreased vision. The channels cross the median raphe temporal to the fovea and drain from the affected to the nonaffected quadrant. The two areas of intense hyperfluorescence (arrows) are as a result of retinal neovascularization. Retinal hemorrhages sometimes resolve over weeks to months, however can persist for years. Hemorrhage blocks fluorescence on angiography and might impair the usefulness of such analysis. Vitreous hemorrhage could develop after rupture of thin, friable neovascular vessels that grow in response to retinal nonperfusion. The majority of eyes with retinal or disk neovascularization will develop vitreous hemorrhage if left untreated. The nearer the nonperfusion is to the macula, the more significant the visible loss might be. When disk neovascularization does happen, retinal neovascularization usually is present as well. The incidence of retinal neovascularization elevated to 36% in eyes with 5 diskdiameters or extra of retinal nonperfusion. Shilling and Kohner reported a 62% incidence of neovascularization among eyes with larger than four disk-diameters of nonperfusion and 0% amongst eyes with less nonperfusion. They usually form following posterior retinal breaks attributable to fibrovascular proliferation and traction. In diabetic retinopathy, the retinal findings are generally bilateral and involve all 4 quadrants. Distinguishing characteristics of hypertensive retinopathy embody bilateral narrowed retinal arterioles and hemorrhages that involve the complete fundus. Available information regarding lots of the reported treatment modalities are based on case series with out controls or randomization. As our Retinal Venous Occlusive Disease understanding of the illness improves, the standard of care is prone to proceed to evolve. If residual fluorescein leakage is observed, another session of grid laser photocoagulation may be indicated. Systemic analysis of commonly related danger factors is a crucial part of the examination course of. However, in patients beneath age 50 years or with bilateral vein occlusions, a more thorough work-up could additionally be warranted. Initial evaluation may include testing for hypertension, diabetes, and a hypercoagulable state. Initial testing might embrace a fasting blood glucose level, complete blood count with differential and platelets, coagulation studies, and erythrocyte sedimentation rate.
Cheap fincar 5mg overnight delivery
Factors leading to weak spot embrace extreme episcleral cautery; tearing or buttonholing of the roof of the tunnels; false passages in the scleral tunnel itself; excessive handling; or heating from the phacoemulsification tip, causing a corneoscleral burn. The latter, in turn, may be attributable to insufficient chamber inflation on the conclusion of surgery, sluggish ciliary body operate (itself usually attributable to hypotony), or accidental wound lip compression. Fechner and Wichman reported a 10% incidence of wound dehiscence in 100 myopic eyes treated with high-dose systemic steroids directly before and after implantation of iris-fixated lenses. The definitive analysis is made by the Seidel take a look at, instilling concentrated fluorescein, using either fluorescein strips or 2% fluorescein resolution. Wound leaks which would possibly be famous within the first day or two postoperatively usually seal on their own as a end result of the postoperative inflammatory process. Inadvertent filtering bleb A wound leak under sealed conjunctiva results in the formation of a filtering bleb. This course of may be hastened using the medical measures mentioned earlier for administration of a wound leak. Filtering blebs that develop after the primary a number of postoperative days usually reflect the breakdown of an initially wellapposed wound, which may occur from trauma, suture breakage or loosening, or scleral melting. Blebs that persist for greater than several days can endure epithelialization of the fistulous tract. This channel is immune to medical treatment and heaps of forms of surgical intervention. Corneal dellen can form adjoining to giant blebs and could be proof against normal therapy with topical lubricants. Closure of a long-standing filtering bleb is sophisticated by epithelialization of the fistula. It is advisable to warn patients with persistent filtering blebs of the chance of bleb-induced endophthalmitis. The incidence and severity of endophthalmitis following cataract surgical procedure is elevated in sufferers with filtering blebs, and early detection is clearly fascinating. Surgical repair consisted of excision of cystic conjunctiva, scraping of fistulous observe, closure of the monitor with interrupted 9-0 nylon sutures, and coverage of the observe with a halfthickness scleral flap. Indeed, the quantity of harm to the wound is nearly all the time rather more widespread than is obvious preoperatively. There is a few controversy over the administration of an iris that has been prolapsed for more than 24 h because of concern in regards to the introduction of epithelium or microorganisms; excision may be most popular in these cases. Presumed traumatic wound dehiscence that was detected 3 weeks following uncomplicated extracapsular cataract extraction. This situation can start at any time in the first 2 years postoperatively and might progress for years thereafter. For most patients, glasses or, in rare cases, contact lenses are adequate treatment. Astigmatic keratotomy or laser keratorefractive surgery is obtainable to sufferers who poorly tolerate the sturdy refractive correction required or who keenly desire improved uncorrected imaginative and prescient. Pathophysiology the ultimate common pathway of corneal stroma edema after cataract surgery is inadequate endothelial pump perform to keep the corneal stroma and epithelium in their relatively dehydrated and clear state. The corneal endothelium acts to dehydrate the cornea both actively by way of an adenosine triphosphate-driven bicarbonate ion pump,39 and passively, by way of the integrity of the mobile membrane barrier. Surgical trauma is commonly the wrongdoer in surprising postoperative corneal endothelial decompensation. Diffuse edema could result from problem in delivering the nucleus in extracapsular cataract extraction or extended ultrasound usage in phacoemulsification, significantly if all or part of the nucleus is fragmented in the anterior chamber. A excessive volume of balanced salt answer infusion alone is mostly nicely tolerated by the corneal endothelium, but extended infusion research have demonstrated a difference between common balanced salt resolution and enhanced balanced salt solution formulation in endothelial damage. It is regularly however not at all times accompanied by other evidence of intraocular toxicity, most notably a fixed and dilated pupil. Care must be taken to use preservative free lidocaine because the preservative, methylparaben has been related to corneal toxicity. For example, a subconjunctival bolus superiorly overlying a superior corneal scleral tunnel may be expressed into the anterior chamber through lid strain. Aminoglycoside antibiotics, in particular, have profound retinal toxicity at all however extremely low concentrations.
Buy 5 mg fincar mastercard
It may occur after disappearance of the hydration 10�15 min after surgical procedure if the construction of the wound was improper. Wound leak on the first postoperative day may enhance the risk of endophthalmitis 44-fold. Wound leak could additionally be handled by hydration of the wound beneath slit lamp after topical anesthesia or suture addition and povidone iodide 2. It is formed due to metaplasia and proliferation of cortical lens fibers that remained on the posterior capsule. Topical corticosteroids could additionally be given for every week to lower intraocular irritation and the patient could additionally be examined a day and per week after the procedure with pupil dilation to rule out retinal detachment. Radial laser capsulotomy or surgical capsulectomy may be performed if the capsulorrhexis is contracted (capsulophimosis or capsular contraction syndrome), as and when that is identified. No distinction in postoperative corneal edema requiring corneal transplantation was reported in different extraction methods. The outcomes of those two approaches are equivalent, however twoincision surgical procedure increases the period of the surgical procedure. If one incision is selected, following scraping of the corneolimbal epithelium on the supposed surgical site, a fornix base conjunctival flap is raised in the upper quadrant. The shock waves propagate and exit by way of the tip port, which also aspirates the fragments. This nonvibrating tip allows safer removing of the nucleus and reduces potential damage to the iris and the posterior capsule. The diameter of the laser tip is smaller than the phacoemulsification tip and requires a smaller incision (1. The system is air-cooled, and the probe generates less warmth than present phacoemulsification machines. The endonucleus could also be eliminated by guide phacofragmentation as an alternative of phacoemulsification. After hydrodissection and hydrodelineation, the endonucleus is introduced into the anterior chamber using hooks and is fragmented manually with a bisector. The endonucleus is released by hydrodelamination and advancement of the 27-gauge cannula underneath the onerous nucleus. The nucleus may be fractured in the anterior chamber and delivered using a plastic glide. This methodology harbors the risk of posterior capsular tear when the cannula is introduced beneath the endonucleus. Future procedures might embrace endocapsular cataract removal by way of a small capsular puncture or by laser or ultrasonic device106 to allow retention of the complete capsular bag. Intracapsular injection of antimetabolites corresponding to cyclosporine or 5-fluorouracil may inhibit proliferation of lens epithelial cells. A monomer that may polymerize throughout the bag with out warmth launch may be injected. Such lens substitutes should have good elasticity with out leakage from the bag after polymerization. Miyake K, Ota I, Ichiashi S, et al: New classification of capsular block syndrome. Bellucci R, Morselli S, Pucci V, Bonomi L: Nucleus viscoexpression compared with different strategies of nucleus removing in extracapsular cataract extraction with capsulorrhexis. Oshika T, Suzuki Y, Kizaki H, Yaguchi S: Two year clinical study of a delicate acrylic intraocular lens. Masket S: Avoiding problems associated with iris retractor use in small pupil cataract extraction. Adjunct units for managing difficult cases in cataract surgical procedure: capsular staining and ophthalmic viscosurgical gadgets. Lundberg B, Jonsson M, Behndig A: Postoperative corneal swelling correlates strongly to corneal endothelial cell loss after phoacoemulsification. Evaluation of various surgical techniques within the administration of subluxated cataractous lens. Nahra Saad D, Castilla Cespedes M, Martinez Palmer A, et al: Phacoemulsification and lens-iris retropulsion syndrome.