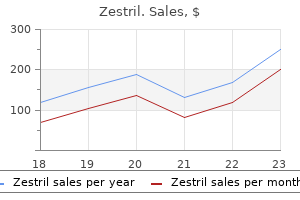
Zestril dosages: 10 mg, 5 mg, 2.5 mg
Zestril packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

Proven 5mg zestril
More than one access may be required when giant tumors are located in different calyces. The irrigation medium used for bipolar electrodes is normal saline, which minimizes the change in serum sodium and other electrolyte abnormalities throughout resection. When water is used as an irrigation medium, hyponatremia and other electrolyte abnormalities may happen [26, 27]. With the bipolar loop resection, deep tissue sampling is possible, simply as with the usual monopolar loop [28]. The induced effects on delicate tissue vary between coagulation, vaporization, and incision, relying on the contact versus noncontact mode. The distal fiber tip ought to be directed tangentially in a noncontact mode till the tissue coagulates. This laser penetrates tissue to a depth of approximately 5�6 mm, so bulky tumors are ablated rather more effectively. As the tissue coagulates, the coagulated portion of the tumor is removed with forceps, which exposes deeper parts of the tumor that require additional coagulation. The shallow depth of penetration allows the tissue ablation to be targeted and circumferential lesions to be treated. This physical property leads to minimal thermal injury to the encircling tissue [32]. Tumors in peripheral calyces (A�C) are best approached by direct puncture as far distally within the calyx as attainable. Tumors within the renal pelvis (D) are higher ureter (E) are best approached by puncture to an higher (1) or middle (2) calyx, which permits the scope to be maneuvered within the renal pelvis and down the ureter. Tumors within the lower calyx are approached by decrease calyx puncture (3) (reproduced from Sagalowsky & Jarrett [24], with permission). Resection of tumor could be achieved with monopolar or bipolar loop electrodes, or tumors could be ablated with lasers. A giant entry sheath allows a regular resectoscope with slicing loop to be introduced in to the upper urinary tract. The entry sheath maintains a low strain system with irrigation by way of the scope. Broad-based tumors could trigger excessive bleeding and are finest approached with resection of the laser therapy. In addition to resection, electrovaporization can be accomplished with a 200-W pure chopping present of the monopolar gadget [25]. The tumor is sampled for diagnostic purposes and handled by holmium or neodymium laser sources. This can be accomplished by way of a standard nephroscope (C) or with a flexible cytoscope (D) (reproduced from Sagalowsky & Jarrett [24], with permission). A mild flow of irrigation is used to clear tumor particles through the ablative remedy. Particular consideration must be given to ensure that the fiber tip is visible in front of the scope always. One method to reduce perforation is the utilization of a large entry sheath to create a path of low resistance via which irrigant can exit freely. This reduces the stress throughout the accumulating system whereas allowing good visualization. Once the perforation is recognized, the process ought to be stopped and maximal drainage of the upper urinary tract should be accomplished with an internal stent and percutaneous nephrostomy tube. Since the pleural area extends inferiorly to the eleventh or 12th rib posteriorly, the violation of the pleural cavity is a well known complication [38]. Pleural harm is recognized at the end of the process by intraoperative fluoroscopy, and usually the hydrothorax or pneumothorax can be seen. When this is confirmed, it could be managed with postoperative insertion of a chest tube or thoracentesis [39]. A small chest tube (10F) may be placed intraoperatively beneath fluoroscopic steering whereas a patient is still under common anesthesia.
Discount 5 mg zestril mastercard
Isometrics are achieved by mild resistance to the elevators and depressors of the mandible in all excursions, with tongue within the palate and slight inocclusion. Correct deviations in rotation, translation, and protrusion through isotonic resistance three. Create smooth motion with resistance throughout the range via lively correction 1. The joint is stretched in to rotation, translation, protrusion, lateral tour, and longitudinal distraction, to find a way to stop growth of adhesions and/or muscle rigidity/shortening. Patients should feel stretching and some discomfort, short of sharp ache or ripping sensation. The "contract-relax" is an opening exercise consisting of making an attempt maximal intermaxillary opening while utilizing a hand to resist opening and shutting isometrically after which opening somewhat farther. There are particular situations by which the affected person benefits from the assistance of the therapist, primarily instances which have a really sluggish progress, no progress in any respect, or the alternative. Stage I Physiotherapy In most cases, patients start stage I rehabilitation on postoperative day 1. Nevertheless, most patients are discouraged in developing hypomobility habits to forestall the inherent cicatricial tissue formation. Stage I rehabilitation focuses on reducing discomfort, ache, spasms, and inflammation (mainly swelling). The complete physiotherapy is performed in a slow and cozy fashion, in need of any sharp ache. Typically, whatever the outcomes of postoperative manipulation beneath anesthesia, the patients will solely hinge-open 10 to 20 mm (one fingerwidth). The patient is assessed for asymmetry or interruptions in movement, overstretching, and/or inappropriate motion patterns. Patients be taught to appropriate vertical opening, protrusion, and lateral tour actions with the aim of fostering applicable operate. If any disk repositioning or diskopexy was carried out, stage I is maintained for two weeks postoperatively. Opening deviations are corrected by opening to the purpose of deviation/excessive translation and using a hand on the contralateral side to resist the incorrect motion. Once initial correction is achieved, the tongue takes over by inserting the apex in to the palate and controlling vertical opening with out deviation. Close monitoring of the patient will prevent improvement of synovitis and myositis. Advancement of diet can additionally be monitored intently so as to forestall an accelerated detrimental progress. Case-oriented harm prevention, neuromuscular leisure, corporeal mechanics, and stress management to reduce irregular mechanics to the myofascial system are applied. Invariably, these sufferers had undergone open arthrotomy earlier than the minimally invasive procedure. This is suggestive of scarring of the preauricular tissues, inflicting an added quantity of pressure on the nerve branches from joint distention, leading to palsy of the frontotemporal and zygomatic facial rami. It becomes manifest as an atony of the orbicularis oculi and the frontal division of the occipitofrontalis, translated within the partial capacity to elevate the eyebrow and to utterly occlude the superior palpebral, each within the immediate postoperative period. Misplacement of the irrigating cannula or overpressure joint lavage can pressure solutions past the confines of the capsule in to the adjoining tissues. As the magnitude and the period of compression increases, wallerian degeneration becomes apparent. The peripheral fascicles and nerve fibers are affected primarily, whereas more centrally positioned fascicles and nerve fibers may be spared. Should axonotmesis and/or neurotmesis occur during puncture, the one factor obstructing nerve regeneration could be cicatricial tissue, which competes with the axonal cone progress to bridge the hole. The mechanism of entry in to the middle ear is thru either the osseous or gentle tissue exterior auditory meatus.
5 mg zestril otc
Studies suggest that cavitation is 548 Section 4 Shock-Wave Lithotripsy tensile or shear stress. There are two items of proof that strongly assist the argument that stone comminution is a fatigue process. First, the internal construction of stones has been shown to affect how they fragment in lithotripsy [100�103]. Second, usually greater than 1000 shock waves are required to progressively fragment stones in to small enough pieces; the utilization of a number of stress cycles to fracture a material is a basic hallmark of fatigue [97, 98]. The two most commonly cited mechanisms are direct stresses (tension and shear) and cavitation, or some combination of them [93]. Part of the issue in determining which mechanism is in action is that solely restricted data on the material strength of kidney stones has been reported. Of observe is the paucity of information for the tensile and shear power of kidney stones. This is most probably as a outcome of figuring out these properties in brittle materials is fraught with technical difficulties. Further, many of the information have been measured in quasi-static exams, with the stress applied over many minutes, and the results may not be consultant of the material properties when topic to shock waves, the place the stress is applied and removed in microseconds [85]. At present the information on materials power of kidney stones are insufficient for the fracture course of to be described. A jet of fluid may be seen punching through the middle of the bubble toward the metal floor (courtesy of Dr L. It has also been suggested that the stresses imparted by cavitation can act by a spall mechanism [86, 94]. The cracks are nucleated at sites of small imperfections that occur in nearly all materials; these nucleation websites will be present in all kidney stones. The imperfections are sites of "stress concentrations" which, when a shock wave passes, can lead to local stresses far in extra of the typical stress induced by the shock wave [99]. These very excessive stresses can cause the imperfections to grow in to micro-cracks with the passage of a number of shock waves. With subsequent shock waves, the micro-cracks grow in to macro-cracks and finally produce cracks large enough to induce failure. The cracks can be grown either by giant tensile stresses or by massive shear stresses. Therefore, fatigue might be enhanced wherever areas of high stress coincide with weak points in the stone. The clinical implications of such adverse effects are nonetheless beneath investigation and an intensive discussion of the issues related to lithotripsy is given in Chapter 53. The notion that lithotripter shock waves can cross harmlessly via the body is simply not true. It is in all probability going that each one sufferers who obtain at least an average dose of shock waves (2000 shock waves at mid-range power or higher) experience some degree of tissue trauma. Lithotripsy has been very beneficial for numerous sufferers, however it has also led to severe, even catastrophic opposed results for others [9, eleven, 108]. To better perceive how shock waves have the potential to trigger tissue trauma, the physics of the issue needs to be thought-about. Although shock waves are targeted on to the stone, the encircling tissue is also subject to significant mechanical forces. In addition, patient motion, as a end result of respiration or discomfort, doubtless results in the stone spending an excellent portion of the therapy outing of the focal region and, thus, most of the shock waves will interact solely with tissue. Fortunately, tissue has physical properties that make it far much less prone to damage by shock waves than kidney stones. For example, the reality that the acoustic impedance of tissue is close to that of water implies that shock waves can move via a tissue�water interface without important reflection. However, tissue is subject to deformation by the strain wave and to cavitation induced by the tensile part of the shock wave.
Best zestril 2.5 mg
Caused by incapability of kidneys to excrete an acceptable amount of acid; this is caused by too few functional nephrons quite than a particular acid secretory defect. Renal failure can result in an anion gap metabolic acidosis as nicely as a traditional anion gap acidosis if due to renal tubular acidosis. Due to overproduction of lactic acid via anaerobic respiration � this typically happens with tissue hypoperfusion and hypoxia but also can occur in states associated with excessive O2 demand. Renal hypoperfusion resulted in a low glomerular filtration price, which reduced the acid excretory capacity of the kidneys. In these conditions, not solely is there extra manufacturing of lactic acid however conversion of lactic acid to glucose by the liver can be decreased because of lowered hepatic blood circulate. In the absence of insulin, "runaway" lipolysis occurs within the adipose tissue, and b-oxidation happens in the liver. This acidosis is further exacerbated by the hyperglycemia, as a outcome of the hyperglycemia causes an osmotic diuresis which results in quantity depletion. Salicylic acid toxicity can cause tinnitus, vertigo, and nausea and in extreme instances may cause seizures and demise; in youngsters and adolescents, it could also cause Reye syndrome. In phrases of acid-base disturbances, salicylic acid toxicity can cause a respiratory alkalosis by stimulating the medullary respiratory heart, inflicting hyperventilation, and a metabolic acidosis by inhibiting oxidative metabolism. The toxic results of the metabolites of methanol could be prevented by competitively inhibiting the enzyme alcohol dehydrogenase with ethanol or fomepizole. Ethylene glycol is a sweet-tasting natural compound incessantly utilized in automotive antifreeze. Most widespread cause of regular anion hole metabolic acidosis Ethylene glycol: sweettasting substance current in antifreeze Anion hole acidosis � urine with oxalate crystals and/or Woods lamp fluorescence! Volume depletion additionally stimulates the renin-angiotensin-aldosterone system; the increased aldosterone promotes Na� reabsorption in change for K� and H� in the distal tubule. Classically characterised by volume expansion, hypertension, hypokalemia, hypernatremia, and metabolic alkalosis. His symptoms improve dramatically, however his urine output drops precipitously on the third day, and his urine specific gravity signifies concentrated urine. Although in this case the hypoventilation resulted in appropriate respiratory compensation, recall that the ability of the lungs to compensate for a metabolic alkalosis is restricted as a outcome of significant hypoventilation will cause hypoxemia. The kidneys are capable of compensate much more successfully for a persistent respiratory acidosis than for an acute respiratory acidosis. Causes of Respiratory Alkalosis Mechanical air flow Pulmonary embolism High-altitude respiration Pneumonia Asthma Drugs. The patient has had current surgery (endothelial trauma) and has doubtless been motionless in bed for several days (stasis). Moreover, her dyspnea is abrupt in onset, and she is hypoxemic with an A-a gradient of 20 mm Hg. A word of caution right here: although the historical past here is traditional for abrupt development of pulmonary embolism, research have shown that sufferers with pulmonary embolism can current with respiratory alkalosis, respiratory acidosis, metabolic acidosis, and without hypoxemia. If third spacing results in important accumulation of fluid in compartments such because the peritoneal cavity or pleural space, the transcellular fluid volume becomes pathologically elevated and the effective circulatory volume could turn into pathologically reduced, leading to tissue hypoperfusion and prerenal azotemia. Approximately 98% of total body potassium is situated inside cells; this potassium can play an important role in buffering of a metabolic acidosis. The massive quantities of proteins are needed for cellular operate and likewise play an important buffering and osmotic function. Treatment of each situations involves inhibition of the pathologically stimulated reninangiotensin-aldosterone neurohormonal cascade. The renin-aldosterone-angiotensin system is probably an important of those mechanisms. In cirrhosis, fluid sequestration in ascitic fluid and within the dilated splanchnic bed ends in a markedly expanded extracellular quantity. The improve in sympathetic outflow alters the circulatory system in several methods: � It increases cardiac contractility and coronary heart rate, thereby rising cardiac output. Assessment of fetal respiration, gross body movements, fetal tone, reactive fetal heart price and amniotic fluid.
Zestril 5mg for sale
They are equally distributed between men and women, the right and left kidneys, and the upper and decrease poles of the kidney. Anatomic studies prior to now have demonstrated an in depth anatomic affiliation between the tributaries of the renal vein and the calyceal fornix. These venous sinuses are near the surface on the calyceal fornix and may erode or rupture via the urothelium [14]. It has been postulated that these venous calyceal fistulas develop following periods of elevated stress inside the intrarenal amassing system [8]. They could also be localized or diffuse, and have been described as venous ruptures, varices, renal forniceal hemorrhages, pyelovenous fistula, and hemorrhagic papillitis. They are among the more widespread causes of bleeding in sufferers with benign important hematuria. Usually, these lesions are found in the kidney, rarely the ureter, and are equally distributed between men and women, right and left kidneys, and higher and decrease poles. Ureteroscopic analysis and therapy are extra profitable when the patient is actively bleeding, and when the lesions are discrete somewhat than diffuse. Despite no bleeding lesion being discovered, most research report successful decision of the hematuria after ureteroscopy. It has been instructed this might be as a result of resolution of unseen venous�calyceal communication due to increased intraluminal pressure during the ureteroscopy [16, 21]. Results with ureteroscopy for the analysis and remedy of benign important hematuria are offered in Table 40. Overall, the success rate for patients being handled ureteroscopically for benign important hematuria is 90%. Technique the first aim of diagnostic ureteroscopy is to get hold of unhindered visual inspection of the whole upper urinary tract. Some authors have reported performing versatile ureteroscopy without a working or a security guidewire. This is possible with some newer flexible ureteroscopes that can be launched in to the ureteral orifice beneath direct vision without the use of a working guidewire [24]. Irrigation with a dilute distinction blended in normal saline permits precise documentation and navigation throughout the intrarenal collecting system. The intrarenal amassing system is inspected from the upper pole, shifting systematically by way of the calyces to the decrease pole, and every calyceal inspection is documented fluoroscopically. Care ought to be taken to avoid over-distention of the intrarenal collecting system to reduce urothelial trauma. Any trauma from the guidewire, over-distention, or ureteroscope can stop correct visualization of those lesions. Likewise, prestenting ought to be avoided to stop stent-related irritation of the urothelium, which also will forestall accurate inspection of the upper urinary tract. Ureteroscopy is actually an endoscopic extension of cystoscopic rules to the higher urinary tract. Ureteroscopic inspection of the higher urinary tract allows direct visualization and recognition of pathologic lesions, just as cystoscopy permits visual recognition of calculi, neoplasms, and other urothelial lesions. Visual inspection of the higher urinary tract by way of endoscopy permits visible recognition and differentiation of upper urinary tract pathology. Ureteroscopic sampling for cytologic and pathologic analysis tremendously improves our capability to distinguish malignant from benign soft tissue lesions. Direct, exact biopsy, guided by ureteroscopic visualization of the lesion, permits a more accurate analysis than a brush biopsy guided by fluoroscopy alone. Biopsy of any suspicious lesions can be performed with 3F biopsy forceps for sessile lesions, or flat wire baskets for papillary lesions [6]. When treating patients with benign important hematuria, when a source of bleeding is discovered, it ought to be fulgurated. Cystourethroscopy Careful and complete 30� and 70� lens Bladder lavage for cytology Visualize ureteral efflux Localize gross hematuria when current Remove cystoscope Rigid ureteroscopy Direct insertion of ureteroscope with no wire Leave wire through the ureteroscope to the level inspected Remove inflexible ureteroscope Flexible ureteroscopy Over the beforehand placed wire Inspect proximally from the level reached with rigid ureteroscope Systematic inspection of intrarenal accumulating system Aspirate intrarenal urine for cytology Biopsy any suspicious lesions Lavage for cytology after biopsy Fulgurate any bleeding lesion Remove flexible ureteroscope and stent as indicated iliac vessels. Just sufficient irrigation is used to provide adequate distention of the ureter for visualization while stopping over-distention of the ureter and intrarenal amassing system. Even minimal over-distention of the amassing system can lead to small areas of urothelial hemorrhage and render the remaining inspection of the ureter for true sources of bleeding pointless. Once the distal ureter is totally inspected to the level of the iliac vessels, further inspection of the proximal ureter requires versatile ureteroscopy.
Discount 2.5mg zestril with amex
These can vary from symptoms of a weak and intermittent urine stream, urgency, urgency incontinence, overflow incontinence, and nocturia, to barely any urination at all. Finally, patients may discover somewhat profound will increase in their urine output, out of proportion to their fluid intake, which ends from poor renal concentrating ability. The urogram can provide each functional and anatomic details of the obstruction, versus ultrasonography, which provides extra anatomic element. Chronic circumstances of ureteral obstruction are normally visualized by ureteral dilation, tortuosity, and a standing column of distinction within the ureter to the point of obstruction. The kidney might reveal marked parenchymal thinning (either segmental or complete), calyceal crescents, and the cleaning soap bubble nephrogram [8]. Obstruction is often associated with an belly mass, usually suprapubic, however it might even be a big flank mass, palpable throughout physical examination, which on rare events can be visible. The patient may also have signs of quantity overload, similar to bipedal edema, pulmonary congestion, and hypertension. Laboratory data could embrace hematuria (microscopic and/or gross), proteinuria, crystalluria, pyuria, and urinary casts. When chronic obstruction is the predominant clinical image, the urinary diagnostic indices are most often just like those seen with acute tubular necrosis: an elevated urinary sodium con- Chapter 7 Pathophysiology of Urinary Tract Obstruction ments. Significant data can be obtained about each the renal parenchyma and the collecting system with no publicity to radiation, or contrastinduced nephrotoxicity or anaphylaxis. Hydronephrosis will appear as a dilated collecting system separating the usually echogenic renal sinus, creating an anechoic central area surrounded by parenchyma. Echoes inside the amassing system could indicate an an infection (pyonephrosis), hemorrhage, or a lesion of the transitional mucosa, among other diagnoses. There are a quantity of pitfalls to using ultrasonography for diagnosing obstruction. Sonograms may be false negative because of an acute onset of obstruction, an intrarenal amassing system, dehydration, and the misinterpretation of caliectasis for renal cortical cysts. Sonograms can be false optimistic for obstruction because of a capacious extrarenal pelvis, parapelvic cysts, vesicoureteral reflux, and a high urine circulate state [8]. Therefore, though an excellent software for the preliminary evaluation of selected patients with suspected renal obstruction, the sonogram ought to be interpreted fastidiously and should be according to the general scientific image. The strategy of affected person preparation and the timing of the administration of the diuretic, when diuretic renography is carried out, are extremely important. In the presence of a lowered creatinine clearance, it could be essential to enhance the diuretic dose to achieve an sufficient flow fee and cut back the chance of a false-negative result [13]. The timing of the administration of the diuretic after the administration of the radiopharmaceutical agent has been fastidiously worked out. The conventional diuretic renogram is performed by administering the radiopharmaceutical agent and obtaining pictures, adopted 20 min later by intravenous administration of the diuretic, after which measuring the half-life for the clearance of the tracer from the amassing system. It provides a noninvasive measure of the relative renal perform and has the flexibility to wash out the radiopharmaceutical agent from the dilated amassing system. It is mostly accepted that a clearance of the radiopharmaceutical agent from the renal pelvis with a half-life of less than 10 min is regular; some specialists think about a halflife of lower than 15 min to be normal. Clearance of tracer with a half-life between 15 and 20 min is considered equivocal and a half-life greater than 20 min signifies an obstruction [9, 18]. Whitaker test the Whitaker take a look at was thought of the gold standard for the analysis of higher urinary tract dilation. It supplied urodynamic evidence of a mechanical obstruction of the upper urinary tract at a given move price. The Whitaker test is performed with the patient placed on a fluoroscopy desk within the susceptible place. Before the affected person is positioned susceptible, a bladder catheter is placed and related to a pressure transducer for continuous monitoring of intravesical pressures with adjustments in renal pressure. A mixture of saline and contrast is run via the renal cannula at a fee of 10 mL/min.
Buy 5 mg zestril fast delivery
Significant sepsis has been thought of a relative contraindication for neuraxial anesthesia (spinal or epidural) for concern of introducing the infection from the bloodstream to the intrathecal space, and causing meningitis; nevertheless, that link has never been clearly established and stays controversial [62]. Furthermore, affected person comorbidities could affect the surgical and/or anesthetic method to the stone. For example, sufferers who must remain on dual antiplatelet therapy perioperatively for prevention of intracoronary stent thrombosis prohibit neuraxial blockade. Also, many myelopathic patients with persistent nephrolithiasis may have developed tolerance to opioids because of continual use, which complicates their anesthetic management and recovery. In patients with severe cardiac disease, sudden hemodynamic changes have to be prevented. Rapid restoration, nonetheless, relies upon enough redistribution and elimination of those brokers, in addition to their lively metabolites. Excretion of those active metabolites is basically dependent upon sufficient renal operate. When radiographic contrast brokers are used, the chance of allergic reactions to the iodinated dyes should even be thought of. Furthermore, latex allergy have to be strongly suspected in myelopathic sufferers who repeatedly self-catheterize to relieve urinary retention, and the operating room have to be ready as a latex free surroundings. Due to repeated exposures, these patients could also be at excessive risk for anaphylaxis at any point through the process [65, 66]. Multiple renal punctures and renal pelvic perforation are associated with a twofold larger blood loss [68]. Many sufferers with nephrolithiasis have a number of comorbidities that have to be considered. Ureteroscopy beneath spinal versus basic anaesthesia: morbidity and stone clearance. American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines on Perioperative Cardiovascular Evaluation for Noncardiac Surgery); Fleisher, L. Executive abstract: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines on Perioperative Cardiovascular Evaluation for Noncardiac Surgery). Ureteroscopic lithotripsy under native anesthesia: analysis of the effectiveness and patient tolerability. Ureteroscopy as an out-patient process: the Singapore General Hospital Urology Centre experience. Percutanous nephrolithotomy underneath general versus combined spinalepidural anesthesia. Impact of body mass index on cost and scientific outcomes after percutaneous nephrostolithotomy. Lung ventilation and perfusion in susceptible and supine postures with reference to anesthetized and mechanically ventilated wholesome volunteers. Blood utilisation in elective basic surgical procedure circumstances: requirements, ordering and transfusion practices. American Society of Anesthesiologists Task Force on Preanesthesia Evaluation: Practice advisory for preanesthesia analysis: a report by the American Society of Anesthesiologists Task Force on Preanesthesia Evaluation. Preoperative laboratory screening in wholesome Mayo patients: cost-effective elimination of checks and unchanged outcomes. Reduction of postoperative mortality and morbidity with epidural or spinal anaesthesia: outcomes from overview of randomised trials. Comparative results of extracorporeal shock wave lithotripsy and percutaneous nephrolithotomy. Complications of extracorporeal shock wave lithotripsy and percutaneous nephrolithotomy. Urolithiasis in patients with spinal cord injuries: threat components, management, and outcomes. College of Cardiology/American Heart Association Task Force on Practice Guidelines. Preoperative pulmonary evaluation: identifying and reducing dangers for pulmonary problems. A combined "civil� mechanical�electrical�electronic�biomedical" combined effort is required, coordinated by the wants, preferences, and safety of the medical/surgical team.
Trusted zestril 2.5 mg
None of the revealed series has evaluated the function of maintenance remedy, doubtless because of entry problems. Randomized multicenter trials are needed to evaluate the function of adjuvant topical remedy. Diagnosis is predicated on microscopic examination of urine and specific fungal culture. Histopathologic examination of fungal balls (accretions) will show the fungus. The polymerase chain response has been used to detect candidemia in patients with candiduria, earlier than the culture reviews are available [113, 114]. Opportunistic pathogens, corresponding to Candida, Aspergillus, Mucor, Cryptococcus, and Histoplasma, in particular are identified to infect the kidneys in predisposed people with serious issues. These infections are often insidious and their diagnosis is usually delayed because of the coexisting illnesses [115, 116]. Renal involvement by fungi has been discovered to be related to elevated morbidity and mortality, significantly in cases of infections by angioinvasive fungi corresponding to Aspergillus and Mucor [117�119]. Fungal infection may be systemic with secondary involvement of the urinary system, or it may originate in the urinary tract after which disseminate hematogenously. The use of an indwelling urethral catheter and administration of a quantity of antibiotics increases the danger of dissemination of urinary fungal infections [120]. These infections of the urinary tract should be recognized quickly and treated aggressively. These fungal balls trigger hydronephrosis, oliguria and even anuria, destruction of renal parenchyma, widespread dissemination of the organism, and demise of the patient [124]. Percutaneous antifungal irrigation permits administration of highly poisonous antifungal medicine to patients with localized an infection, thereby minimizing systemic unwanted aspect effects [125, 126]. Systemic antifungal brokers have been efficiently used, however within the presence of an obstructed kidney because of in depth fungal infection, drainage of the pelvicalyceal system is obligatory to salvage the kidney. Amphotericin B and its formulations, the azoles (fluconazole, itraconazole, voriconazole, and ketoconazole), caspofungin, and flucytosine are used to deal with urinary fungal infections. Schelenz and Ross reported that the intravenous antifungal medicine, similar to caspofungin or amphotericin B, are useful in treating or preventing candidemia during instrumentation, similar to insertion of nephrostomy tubes in cases of Candida pyonephrosis [2]. Conservative administration also needs to embody native drainage of pus and fungi as properly as instillation of an effective antifungal agent. The dialogue below is limited to the main drugs used as topical urinary antifungals, specifically fluconazole and amphotericin B. It must be stored in mind that fungal infections involving the genitourinary tract are regularly part of a multiorgan systemic disease in an immunocompromised host. The drug inhibits the cytochrome P-450 enzyme liable for conversion of lanosterol to ergosterol, the main sterol of most fungal cell membranes. Fluconazole is highly water soluble and could be administered intravenously or orally. It is cleared primarily by renal excretion, with approximately 80% of the dose excreted as unchanged drug [127]. Fluconazole administered by mouth or intravenously achieves excessive urine ranges [128]. In one collection, orally administered fluconazole (100 mg twice every day for 10 days) eradicated candiduria in 19 of 20 critically sick patients, which was comparable to amphotericin B bladder irrigations [129, 130]. It is essential to observe that an elevated serum creatinine value is related to a reduced price of fungal eradication from the urine with systemic fluconazole therapy. This is likely related to lower urinary levels of fluconazole in sufferers with reduced renal operate [131]. Therefore, in patients with renal impairment, direct irrigation may be simpler at treating candiduria. Others have advocated that amphotericin B not be used in the management of candiduria [129]. Removal of the urinary catheter, if possible, is extra helpful for the patient than instillation of bladder irrigation with amphotericin B [144]. Schelenz and Ross demonstrated the limitation of intravenous antifungal brokers such as caspofungin as the sole treatment of an obstructive higher urinary tract an infection because of Candida species [2]. In order to achieve long�term sustained cure from an obstructive pyonephrosis, pus and fungal balls should be drained and an antifungal agent such as amphotericin B deoxycholate instilled locally.