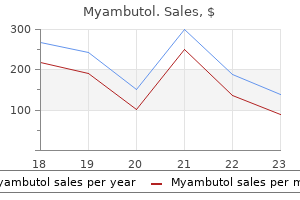
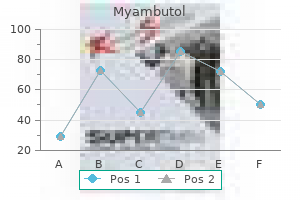
Myambutol dosages: 800 mg, 600 mg, 400 mg
Myambutol packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

Effective myambutol 400mg
High circulate rates (up to 200 mL/kg/ min) may be necessary to guarantee adequate perfusion in very young patients. Intraoperative echocardiography, together with measurement of the stress and oxygen saturation inside the numerous chambers, could reveal the problem. Calcium salts are more typically useful in critically ill younger sufferers than in adults as children more often have impaired calcium homeostasis; ionized calcium measurements are invaluable in such circumstances. Close monitoring of glucose is required as a result of both hyperglycemia and hypoglycemia may be noticed. Dopamine and epinephrine are essentially the most generally used inotropes in pediatric sufferers. Inhalation nitric oxide may be useful for refractory pulmonary hypertension. At a core temperature of 15�C, as much as 60 min of complete circulatory arrest could additionally be protected. Ice packing across the head is used to delay rewarming and for floor cooling of the mind. Pharmacological brain safety is commonly tried with methylprednisolone, 30 mg/kg, and mannitol, zero. Patients present process intensive or sophisticated procedures will usually stay intubated. Extubation may be thought of for older, comparatively healthy sufferers present process easy procedures similar to closure of a patent ductus or atrial septal defect or restore of coarctation of the aorta. The process is generally related to 80% to 90% postoperative survival at 1 12 months and 60% to 90% survival at 5 years. Transplantation improves quality of life, permitting most patients to resume a relatively regular life-style. Unfortunately, the variety of cardiac transplants performed is restricted by the supply of donor hearts, which are obtained from brain-dead patients, most commonly following intracranial hemorrhage or head trauma. Intractable heart failure may be the outcomes of a extreme congenital lesion, ischemic cardiomyopathy, viral cardiomyopathy, peripartum cardiomyopathy, a failed prior transplantation, or valvular heart illness. Other medication could include diuretics, vasodilators, and even oral inotropes; oral anticoagulation with warfarin can also be necessary. Patients may not be able to survive without intravenous inotropes while awaiting transplantation. Transplant candidates must not have suffered intensive end-organ injury or have other main systemic illnesses. Reversible kidney and hepatic dysfunction are frequent due to chronic hypoperfusion and venous congestion. Patients with longstanding pulmonary hypertension may, nevertheless, be candidates for mixed heart�lung transplantation. Premature induction of anesthesia unnecessarily prolongs the time beneath anesthesia for the recipient, whereas delayed induction may jeopardize graft function by prolonging the period of ischemia. Patients might obtain little advance warning of the provision of a suitable organ. Many could have eaten a recent meal and must be thought of to have a full abdomen. Administration of a clear antacid (sodium citrate), a histamine H2-receptor blocker, and metoclopramide must be thought of. Any sedating premedication may be administered intravenously simply prior to induction. Induction could also be carried out with small doses of opioids (fentanyl, 5�10 mcg/kg) with or without etomidate (0. Aminocaproic acid or tranexamic acid can be utilized to decrease postoperative bleeding. If a pulmonary artery catheter was placed, it should be fully withdrawn from the center with its tip within the superior vena cava. Although the transplanted coronary heart is completely denervated and direct autonomic influences are absent, its response to circulating catecholamines is often regular.
Order cheap myambutol line
In the case of laparoscopic surgery, the surgeon must be asked to verify and to decrease insufflation pressure. Indigo carmine was given intravenously, and the proximal finish of a severed left ureter was subsequently identified. Does perioperative hemodynamic optimization defend renal function in surgical patients Renal angina: Concept and development of pretest likelihood assessment in acute kidney damage. The incidence and risk elements of acute kidney damage after hepatobiliary surgical procedure: A prospective observational research. Immediate consequences of acute kidney damage: the influence of conventional and nontraditional complications on mortality in acute kidney damage. Acute kidney harm in the perioperative interval and in intensive care units (excluding renal alternative therapies). Acute kidney harm after lung resection surgery: Incidence and perioperative threat factors. Incidence, predictive factors, and scientific outcomes of acute kidney injury after gastric surgical procedure for gastric cancer. Variations in the danger of acute kidney injury throughout intraabdominal surgical procedure procedures. Risk factors of postoperative acute kidney damage in patients present process esophageal cancer surgical procedure. Acute kidney harm following cardiac surgical procedure: Current understanding and future instructions. Acute kidney damage in the critically unwell patient: A current review of the literature. Intra-abdominal hypertension and stomach compartment syndrome: An underappreciated explanation for acute kidney injury. Association of intraoperative hypotension with acute kidney injury after elective noncardiac surgical procedure. Acute kidney injury after main stomach surgery: A retrospective cohort evaluation. Acute kidney damage is surprisingly frequent and a powerful predictor of mortality in surgical sepsis. Creatinine clearance measurement is the most accurate technique obtainable for clinically assessing total kidney function. The accumulation of morphine and meperidine metabolites has been reported to extend respiratory despair in patients with kidney failure. Succinylcholine could be safely utilized in sufferers with kidney failure in the absence of hyperkalemia at the time of induction. Extracellular fluid overload from sodium retention, in association with increased cardiac demand imposed by anemia and hypertension, makes sufferers with endstage kidney illness notably susceptible to congestive coronary heart failure and pulmonary edema. Controlled air flow should be thought-about for patients with kidney failure underneath basic anesthesia. Inadequate spontaneous or assisted ventilation with progressive hypercarbia under anesthesia can lead to respiratory acidosis that may exacerbate preexisting acidemia, result in probably extreme circulatory depression, and dangerously increase serum potassium concentration. Intravascular quantity depletion, sepsis, obstructive jaundice, crush injuries, and renal toxins, similar to radiocontrast brokers, certain antibiotics, angiotensin-converting enzyme inhibitors, and nonsteroidal antiinflammatory medication, are main risk factors for acute deterioration in kidney operate. The use of mannitol, low-dose dopamine infusion, loop diuretics, or fenoldopam for kidney safety is controversial and with out proof of efficacy. It is a systemic dysfunction that can embrace fluid and electrolyte derangements, respiratory failure, major cardiovascular occasions, weakened immunocompetence leading to infection and sepsis, altered psychological standing, hepatic dysfunction, and gastrointestinal hemorrhage. Evaluating Kidney Function Impaired kidney perform could also be as a end result of glomerular dysfunction, tubular dysfunction, or urinary tract obstruction. Creatinine Clearance (mL/min) Normal Decreased kidney reserve Mild kidney impairment Moderate kidney insufficiency Kidney failure End-stage kidney disease1 1 100�120 60�100 40�60 25�40 <25 <10 this time period applies to sufferers with chronic kidney failure. Diagnosis of acute kidney damage: Kidney Disease Improving Global Outcomes criteria and past.
Syndromes
- Transfusion reaction
- Childbirth
- Stomach ache
- Hepatitis B
- Problems with your eyesight
- Vaginal discharge with abnormal color, texture, or smell
Buy cheap myambutol 800 mg online
Tidal volumes of 6 mL/kg, with prolongation of the expiratory time, might allow extra uniform distribution of fuel flow to both lungs and will assist keep away from air trapping. The disorder is strongly related to cigarette smoking and has a male 5 predominance. The chronic airflow limitation of this disease is because of a mixture of small and enormous airway illness (chronic bronchitis/ bronchiolitis) and parenchymal destruction (emphysema), with illustration of these two parts varying from patient to affected person. In many sufferers, the obstruction has an element of reversibility, presumably from bronchospasm (as proven by improvement in response to administration of a bronchodilator). With advancing disease, maldistribution of each ventilation and pulmonary blood circulate ends in areas of low (V/Q) ratios (intrapulmonary shunt), as nicely as areas of high (V/Q) ratios (dead space). Bronchospasm must be treated by increasing the focus of the unstable agent and administering an aerosolized bronchodilator. Infusion of low-dose epinephrine could additionally be needed if bronchospasm is refractory to different interventions. Intravenous hydrocortisone could be given, significantly in sufferers with a historical past of responding to glucocorticoid remedy. Sugammadex avoids the problem of increasing acetylcholine concentration; nevertheless, instances of allergic reaction to sugammadex have been reported. Chronic Bronchitis the medical prognosis of persistent bronchitis is defined by the presence of a productive cough on most days of 3 consecutive months for at least 2 consecutive years. In addition to cigarette smoking, exposure to air pollution, occupational publicity to dusts, recurrent pulmonary infections, and familial factors may be accountable. Secretions from hypertrophied bronchial mucous glands and mucosal edema from irritation of the airways produce airflow obstruction. Recurrent pulmonary infections (viral and bacterial) are common and infrequently related to bronchospasm. Emphysema Emphysema is a pathological dysfunction characterised by irreversible enlargement of the airways distal to terminal bronchioles and destruction of alveolar septa. Mild apical emphysematous changes are a normal, clinically insignificant consequence of aging. Less commonly, emphysema occurs at an early age and is associated with a homozygous deficiency of 1-antitrypsin. This is a protease inhibitor that forestalls extreme activity of proteolytic enzymes (mainly elastase) in the lungs; these enzymes are produced by pulmonary neutrophils and macrophages in response to infection and pollutants. Emphysema associated with smoking could equally be due to a relative imbalance between protease and antiprotease activities in prone people. The centrilobular (or centriacinar) form results from dilation or destruction of the respiratory bronchioles, is more carefully related to tobacco smoking, and has predominantly an higher lobe distribution. The panlobular (or panacinar) kind ends in a more even dilation and destruction of the entire acinus, is related to 1-antitrypsin deficiency, and has predominantly a decrease lobe distribution. Loss of the elastic recoil that normally helps small airways by radial traction permits untimely collapse during exhalation, leading to expiratory flow limitation with air trapping and hyperinflation (see Table 24�2). Disruption of the alveolar�capillary structure and loss of the acinar structure lead to decreased dif fusion lung capability, (V/Q) mismatch, and impairment of gasoline trade. Also, normal parenchyma might turn into compressed by the hyperinflated parts of the lung, resulting in an extra improve in the (V/Q) mismatch. Destruction of pulmonary capillaries within the alveolar septa leads to the event of mild to reasonable pulmonary hypertension. Inhaled 2-adrenergic agonists, glucocorticoids, and ipratropium are routinely employed. Patients with chronic hypoxemia (Pao2 <55 mm Hg) and pulmonary hypertension require low-flow oxygen remedy (1�2 L/min). Consequently, oxygen remedy is targeted to a hemoglobin oxygen saturation of 90%. Pulmonary rehabilitation could enhance the useful status of the patient by bettering bodily signs and train capability. Many sufferers have concomitant cardiac disease and should also receive a cautious cardiovascular analysis. The risk that postoperative air flow may be necessary in high-risk sufferers should be discussed with both the patient and the surgeon. Smoking ought to be discontinued for a minimal of 6 to eight weeks earlier than the operation to decrease secretions and to scale back pulmonary problems.
Buy generic myambutol 400 mg on-line
Nitrous oxide administration is contraindicated in this circumstance: the bubble will increase in measurement if nitrous oxide is run because nitrous oxide is 35 instances more soluble than nitrogen in blood (see Chapter 8). Thus, it tends to diffuse into an air bubble extra quickly than nitrogen (the main part of air) is absorbed by the bloodstream. Its longer duration of action (up to 10 days) in contrast with an air bubble can present a therapeutic benefit. The bubble measurement doubles inside 24 h after injection, because nitrogen from inhaled air enters the bubble more rapidly than the sulfur hexafluoride diffuses into the bloodstream. If the patient is respiratory nitrous oxide, nonetheless, the bubble will quickly improve in size and should result in intraocular hypertension. A 70% impressed nitrous oxide concentration will virtually triple the dimensions of a 1-mL bubble and should double the strain in a closed eye within 30 min. Subsequent discontinuation of nitrous oxide will lead to reabsorption of the bubble, which has turn out to be a combination of nitrous oxide and sulfur hexafluoride. The consequent fall in intraocular pressure could precipitate another retinal detachment. Complications involving the intraocular expan4 sion of fuel bubbles could be avoided by discontinuing nitrous oxide no much less than 15 min prior to the injection of air or sulfur hexafluoride, or by avoiding the utilization of nitrous oxide completely. Nitrous oxide ought to be avoided till the bubble is absorbed (5 days after air and 10 days after sulfur hexafluoride injection). One drop (typically, roughly 1/20 mL) of 10% phenylephrine accommodates approximately 5 mg of drug. Medications utilized 5 topically to mucosa are absorbed systemically at a price intermediate between absorption following intravenous and subcutaneous injection. The two patient populations more than likely to require eye surgery, pediatric and geriatric, are at specific danger of the poisonous results of topically utilized drugs and will obtain at most a 2. Echothiophate (phospholine iodide) is an irre6 versible cholinesterase inhibitor used in the therapy of glaucoma. Topical software leads to systemic absorption and an inhibition of plasma cholinesterase activity. Epinephrine eye drops may cause hypertension, tachycardia, and ventricular arrhythmias; the arrhythmogenic results are potentiated by halothane. Direct instillation of epinephrine into the anterior chamber of the eye has not been associated with cardiovascular toxicity. Timolol, a nonselective -adrenergic antagonist, reduces intraocular strain by reducing manufacturing of aqueous humor. Topically utilized timolol eye drops, commonly used to treat glaucoma, will usually lead to reduced heart price. In uncommon cases, timolol has been associated with atropine-resistant bradycardia, hypotension, and bronchospasm throughout common anesthesia. General anesthesia is indicated in children and uncooperative sufferers, as even small head actions can prove disastrous throughout microsurgery. Adult sufferers are often elderly, with systemic sicknesses similar to hypertension, diabetes mellitus, and coronary artery illness, and pediatric patients might have related congenital problems. The key to induc7 ing anesthesia in a affected person with an open eye harm is controlling intraocular strain with a clean induction. Specifically, coughing throughout General Anesthesia for Ophthalmic Surgery the choice between common and native anesthesia should be made jointly by the affected person, anesthesiologist, and surgeon. The intraocular pressure response to laryngoscopy and endotracheal intubation may be moderated by prior administration of intravenous lidocaine (1. Endotracheal tube kinking, respiratory circuit disconnection, and unintentional extubation could also be more likely because of the surgeon working near the airway. The risk of arrhythmias brought on by the oculocardiac reflex will increase the significance of closely monitoring the electrocardiogram. In distinction to most other types of pediatric surgical procedure, toddler physique temperature might rise throughout ophthalmic surgical procedure due to head-to-toe draping and minimal physique floor exposure. The ache and stress evoked by eye surgery are considerably lower than during a major surgical procedure. The lack of cardiovascular stimulation inherent in most eye procedures combined with the need for sufficient anesthetic depth can end result in hypotension in aged individuals. This drawback is usually avoided by ensuring enough intravenous hydration and by administering small doses of intravenous vasoconstrictors.
Buy myambutol from india
Following preoxygenation, awake intubation with an armored tracheal tube could additionally be most secure in a cooperative affected person. Use of a versatile bronchoscope is advantageous within the presence of airway distortion and can outline the location and diploma of obstruction. Coughing or straining, however, could precipitate full airway obstruction because the resultant optimistic pleural strain increases intrathoracic tracheal compression. Induction: the goal ought to be a smooth induction sustaining spontaneous ventilation and hemodynamic stability. Using 100% oxygen, considered one of three induction techniques can be utilized: (1) intravenous ketamine (because it ends in greater hemodynamic stability in sufferers with decreased cardiac output); (2) inhalational induction with a volatile agent (usually sevoflurane); or (3) incremental small doses of propofol or etomidate. Positive-pressure ventilation can precipitate severe hypotension, and quantity loading prior to induction could partly offset impaired ventricular filling secondary to caval obstruction. Extubation: At the tip of the process, patients ought to be left intubated till the airway obstruction has resolved, as determined by versatile bronchoscopy or the presence of an air leak across the tracheal tube when the tracheal cuff is deflated. Physiologic analysis of the patient with lung cancer being considered for resection surgical procedure. A comparability of the efficacy and antagonistic results of double lumen endobronchial tubes and bronchial blockers in thoracic surgery: A systematic review and meta-analysis of randomized controlled trials. Lung transplantation: From the procedure to managing patients with lung transplantation. Lung damage after one-lung ventilation; a evaluation of the pathophysiologic mechanisms affecting the ventilated and collapsed lung. Intraoperative ventilation strategies to prevent postoperative pulmonary problems: Systematic review, metaanalysis, and trial sequential analysis. Trends and new proof within the administration of acute and continual post-thoracotomy pain-an overview of the literature from 2005�2015. The cerebral autoregulation curve is shifted to the right in sufferers with persistent arterial hypertension. The motion of a given substance throughout the blood�brain barrier is ruled concurrently by its measurement, cost, lipid solubility, and degree of protein binding in blood. The blood�brain barrier could additionally be disrupted by extreme hypertension, tumors, trauma, strokes, infection, marked hypercapnia, hypoxia, and sustained seizure exercise. Any increase in one component have to be offset by an equivalent decrease in one other to forestall an increase in intracranial pressure. In some cases, these alterations are deleterious, whereas in others they might be useful. This article reviews important physiological concepts and discusses the cerebral results of generally used anesthetics. Because of the rapid oxygen consumption and the absence of significant oxygen reserves, interruption of cerebral perfusion usually results in unconsciousness within 10 s. The more rostral "larger" mind regions (cortex, hippocampus) are more delicate to hypoxic damage than the brainstem. Brain glucose consumption is roughly 5 mg/100 g/min, of which more than 90% is metabolized aerobically. Although the mind can also take up and metabolize lactate, cerebral perform is normally dependent on a steady supply of glucose. Paradoxically, hyperglycemia can exacerbate global and focal hypoxic brain harm by accelerating cerebral acidosis and cellular harm. Adequate management of perioperative blood glucose focus is advocated in part to forestall adverse results of hyperglycemia throughout ischemia; nevertheless, overzealous blood glucose management can likewise produce damage by way of iatrogenic hypoglycemia. An ultrasound probe (2 mHz, pulse wave Doppler) is positioned within the temporal space above the zygomatic arch, which allows insonation of the middle cerebral artery. Velocities higher than one hundred twenty cm/s can point out cerebral artery vasospasm following subarachnoid hemorrhage or hyperemic blood flow. Comparison between the velocities in the extracranial inner carotid artery and the center cerebral artery (the Lindegaard ratio) can distinguish between these conditions. Middle cerebral artery velocity 3 times that of the velocity measured within the extracranial internal carotid artery more likely reflects cerebral artery vasospasm. Decreased saturation is related to impaired cerebral oxygen delivery, although near-infrared spectroscopy primarily displays cerebral venous oxygen saturation. Brain tissue oxygen tensions lower than 20 mm Hg warrant interventions, and values lower than 10 mm Hg are indicative of mind ischemia.
Buy myambutol 800mg visa
However, problems such as airway obstruction, shivering, agitation, delirium, ache, nausea and vomiting, hypothermia, and autonomic lability are incessantly encountered. Patients receiving spinal or epidural anesthesia may experience decreases in blood pressure throughout transport or restoration; the sympatholytic results of main conduction blocks may stop compensatory reflex vasoconstriction when sufferers are moved or once they sit up. As the length of anesthesia will increase, emergence additionally turns into increasingly depending on complete tissue uptake, which is a operate of agent solubility, the average concentration used, and the length of publicity to the anesthetic. Recovery from most intravenous brokers depends primarily on redistribution rather than metabolism and elimination. As the total administered dose will increase, nevertheless, cumulative results turn out to be clinically apparent in the type of prolonged emergence; the termination of motion becomes increasingly depending on the metabolism or elimination. This is the idea for the idea of a context-sensitive half-time (see Chapter 7). They should have expertise in airway management and superior cardiac life support, as properly as in problems commonly encountered in surgical sufferers relating to wound care, drainage catheters, and postoperative hemorrhage. The anesthesia staff emphasizes management of analgesia, airway, cardiac, pulmonary, and metabolic problems, whereas the surgical staff generally manages any issues immediately related to the surgical process itself. A ratio of one recovery nurse for two patients is mostly passable; nevertheless, staffing for nursing care must be tailor-made to the distinctive necessities of every affected person and every facility. If the operating room schedule frequently consists of pediatric patients or frequent short procedures, a ratio of one nurse to one patient is usually wanted. Premedication with brokers that outlast the process (eg, lorazepam) may be anticipated to extend emergence. The quick length of action of midazolam makes it an appropriate premedication agent for brief procedures. Since the switch of intubated patients will at all times embrace the danger of inadvertent endotracheal tube dislodgement, appropriate airway gear and supplies must be included in the switch course of, particularly if the switch travel distance is prolonged or includes an elevator journey. The head-down place is useful for management of hypovolemic patients, whereas the back-up place is beneficial for sufferers with underlying pulmonary dysfunction (see Chapters 20 and 23). Patients at increased risk of vomiting or upper airway bleeding (eg, following tonsillectomy) ought to be transported in the lateral position, which additionally helps stop airway obstruction and facilitates drainage of secretions. Delayed Emergence the most frequent reason for delayed emergence (when the affected person fails to regain consciousness inside an anticipated period of time after general anesthesia) is residual drug effect. The results of preoperative sleep deprivation or drug ingestion (alcohol, sedatives) can be additive to those of anesthetic brokers in producing prolonged emergence. Intravenous physostigmine (1�2 mg) could partially reverse the effect of different agents. Less widespread causes of delayed emergence include hypothermia, marked metabolic disturbances, and perioperative stroke. A core temperature of lower than 33�C has an anesthetic effect and significantly potentiates the actions of central nervous system depressants. Hypoxemia and hypercarbia are readily excluded by pulse oximetry, capnography, and blood gasoline analysis. Hypercalcemia, hypermagnesemia, hyponatremia, and hypoglycemia and hyperglycemia are rare causes of delayed emergence that require laboratory measurements for diagnosis. Perioperative stroke is rare, except after neurological, cardiac, and cerebrovascular surgical procedure (see Chapter 28); prognosis is facilitated by neurological evaluation and radiological imaging. Subsequent blood pressure, coronary heart price, and respiratory fee measurements are routinely made no less than each 5 min for 15 min or till stable, and each 15 min thereafter. Additional monitoring contains evaluation of ache; the presence or absence of nausea or vomiting; and adequacy of hydration and output, together with urine move, drainage, and bleeding. Postoperative orders should handle analgesia and nausea/vomiting remedy; epidural or perineural catheter care, including the need for acute ache service involvement; administration of fluids or blood merchandise; postoperative air flow; chest radiographs for follow-up of central venous catheterization, etc. All sufferers recovering from general anesthesia should receive supplemental oxygen and pulse oximetry monitoring during emergence as a outcome of transient hypoxemia can develop even in wholesome sufferers. Arterial blood fuel measurements could additionally be obtained to affirm abnormal oximetry readings, but are normally not necessary. Patients should generally be nursed in the back-up position to optimize oxygenation. However, elevating the top of the mattress earlier than the affected person is responsive can result in airway obstruction. In such cases, a preexisting oral or nasal airway ought to be left in place till the affected person is awake and in a place to preserve airway. Sensory and motor levels ought to be periodically recorded following regional anesthesia to doc regression of the block.
Helianthemum canadense (Frostwort). Myambutol.
- Are there safety concerns?
- What is Frostwort?
- Dosing considerations for Frostwort.
- How does Frostwort work?
- Digestive problems and ulcers.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96241
Myambutol 400mg for sale
It consists of C-shaped cartilaginous rings, which type the anterior and lateral partitions of the trachea and are connected posteriorly by the membranous wall of the trachea. The cricoid cartilage is the narrowest a part of the trachea, with a median diameter of 17 mm in men and 13 mm in women. The tracheal lumen narrows slightly because it progresses toward the carina, the place it bifurcates into the proper and left mainstem bronchi on the stage of the sternal angle. The right mainstem bronchus continues as the bronchus intermedius after the take-off of the best upper lobe bronchus. The distance from the tracheal carina to the takeoff of the proper upper lobe bronchus is an average of two. One in every 250 individuals in the general inhabitants might have an irregular take-off of the best upper lobe bronchus emerging from above the tracheal carina on the right side. The left mainstem 1 the trachea serves as a conduit for air flow bronchus is longer than the best mainstem bronchus and measures a mean of 5. The left mainstem bronchus divides into the left upper lobe bronchus and the left decrease lobe bronchus. Humidification and filtering of inspired air are capabilities of the upper airway (nose, mouth, and pharynx). An estimated 300 to 500 million alveoli provide an infinite membrane surface space (50�100 m2) for fuel trade within the average grownup. With every successive division, the mucosa makes a gradual transition from ciliated columnar to cuboidal and at last to flat alveolar epithelium. Gas change can happen solely across the flat epithelium, which begins to seem on respiratory bronchioles (generations 17�19). The wall of the airway steadily loses its cartilaginous support (at the bronchioles) after which its smooth muscle. Loss of cartilaginous support causes the patency of smaller airways to turn into depending on radial traction by the elastic recoil of the encircling tissue; as a corollary, airway diameter becomes depending on total lung quantity. Cilia on the columnar and cuboidal epithelium usually beat in a synchronized trend, such that mucus produced by the secretory glands lining the airway (and any related bacteria or debris) moves towards the mouth. In the upright place, the largest alveoli are at the pulmonary apex, whereas the smallest are inclined to be at the base. On the thin side, the alveolar epithelium and capillary endothelium are separated by their respective cellular and basement membranes; on the thick side, where fluid and solute change happens, the pulmonary interstitial space separates alveolar epithelium from capillary endothelium. The pulmonary interstitial house contains primarily elastin, collagen, and nerve fibers. These tight junctions are necessary in stopping the passage of huge oncotically lively molecules such as albumin into the alveolus. These inclusions include surfactant, an essential substance necessary for regular pulmonary mechanics. Neutrophils are additionally typically current in people who smoke and sufferers with pneumonia or acute lung harm. Pulmonary Circulation & Lymphatics the lungs are supplied by two circulations, pulmonary and bronchial. The bronchial circulation arises from the left coronary heart and sustains the metabolic wants of the tracheobronchial tree. The bronchial circulation offers a small amount of blood circulate (ie, <4% of the cardiac output). Branches of the bronchial artery supply the wall of the bronchi and comply with the airways so far as the terminal bronchioles. The capillary is incorporated into the thin (gas-exchanging) facet of the alveolus on the right. The interstitial area is integrated into the thick facet of the alveolus on the left. Below that degree, lung tissue is supported by a mixture of the alveolar gas and pulmonary circulation. The pulmonary circulation normally receives the entire output of the right heart via the pulmonary artery, which divides into right and left branches to provide each lung. The oxygenated blood is then returned to the left coronary heart by four primary pulmonary veins (two from each lung). Although flows through the systemic and pulmonary circulations are equal, the decrease pulmonary vascular resistance ends in pulmonary pressures that are less than those within the systemic vessels; consequently, both pulmonary arteries and veins usually have thinner partitions than systemic vessels with much less easy muscle.

Cheap 600 mg myambutol mastercard
Diagnosis is usually difficult, however is usually recommended by a bleeding diathesis with a low fibrinogen stage but relatively normal coagulation tests and platelet count (as famous next). Patients with usually functioning platelets and platelet counts above 100,000/L have normal major hemostasis. The regular platelet depend is 150,000 to 450,000/L, and the bleeding time is usually not affected by the platelet count when the latter is bigger than a hundred,000/L. When the platelet rely is 50,000/L or greater, extreme bleeding typically occurs solely with extreme trauma or in depth surgical procedure. In contrast, sufferers with platelet counts lower than 20,000/L often develop important bleeding following even minor trauma. Thrombocytopenia normally results from considered one of three mechanisms: (1) decreased platelet production, (2) splenic sequestration of platelets, or (3) elevated platelet destruction. The third mechanism may fall under considered one of two categories of destruction: immune or nonimmune. A extended bleeding time with a standard platelet rely implies a qualitative platelet defect. Although the bleeding time is somewhat depending on the approach employed, values longer than 10 min are generally thought-about irregular. Significant intraoperative and postoperative bleeding may be expected when the bleeding time exceeds 15 min. Increasingly patients with cardiac stents are treated with a wide selection of antiplatelet brokers corresponding to clopidogrel, which impair platelet function for the life of the platelet. Assays of platelet perform can be found to determine the diploma to which platelet function is inhibited. The commonest inherited bleeding dysfunction (1:800�1000 patients) is von Willebrand illness. At least three types of the disease are recognized, ranging in severity from gentle to extreme. What other hereditary hemostatic defects may be encountered in anesthetic practice A bleeding diathesis might exist even in the absence of gross abnormalities on routine laboratory exams. Some hemostatic defects are sometimes not detected by routine testing, however require extra specialized exams. A historical past of excessive bleeding after dental extractions, childbirth, minor surgery, minor trauma, or even during menstruation suggests a hemostatic defect. A family history of a bleeding diathesis could suggest an inherited coagulation defect, but such history is often absent as a end result of the elevated bleeding is usually minor and goes unnoticed. Bleeding in patients with major hemostatic defects normally instantly follows minor trauma, is confined to superficial websites (skin or mucosal surfaces), and infrequently may be controlled by local compression. Small pinpoint hemorrhages from capillaries in the dermis (petechiae) are typically present on examination. Bleeding into subcutaneous tissues (ecchymosis) from small arterioles or venules can additionally be common in sufferers with platelet problems. In contrast, bleeding that outcomes from secondary hemostatic defects is normally delayed following injury, is typically deep (subcutaneous tissues, joints, physique cavities, or muscles), and is often difficult to stop even with compression. Hemorrhages may be palpable as hematomas or might go unnoticed when positioned deeper (retroperitoneal). Most laboratory exams are carried out at body temperature and should not reflect the consequences of hypothermia. Refining the ammonia hypothesis: A pathology-driven strategy to the remedy of hepatic encephalopathy. Practical use of thromboelastometry within the management of perioperative coagulopathy and bleeding. Isoflurane and sevoflurane are the risky agents of alternative for patients with vital liver disease as a result of they preserve hepatic blood circulate and oxygen supply. In evaluating sufferers for persistent hepatitis, laboratory check outcomes could present only a gentle elevation in serum aminotransferase activity and infrequently correlate poorly with illness severity. Liver cirrhosis refers to the damaging effects to the liver of irritation, hepatocellular injury, and the resulting fibrosis and regeneration of hepatocytes. Liver cirrhosis results in portal hypertension, varices, and widespread endothelial harm from toxins not cleared by the liver that will cause multiorgan dysfunction.
Myambutol 600 mg line
The common time from induction of spinal anesthesia to arrest was 36 min, and, in all circumstances, arrest was preceded by a gradual decline in coronary heart fee and blood stress. Just prior to arrest, the commonest signs were bradycardia, hypotension, and cyanosis. Treatment consisted of ventilatory support, ephedrine, atropine, cardiopulmonary resuscitation (average period 10. Despite these interventions, 10 sufferers remained comatose and 4 patients regained consciousness with important neurological deficits. A subsequent study concluded that such arrests had little relationship to sedation, however had been related to intensive levels of sympathetic blockade, with unopposed vagal tone and profound bradycardia. Rapid applicable treatment of bradycardia and hypotension is essential to reduce the danger of profound bradycardia, full coronary heart block, or cardiac arrest. Early remedy of bradycardia with atropine or glycopyrrolate might prevent a downward spiral. Stepwise doses of ephedrine, epinephrine, and other vasoactive drugs should be given to deal with hypotension. If cardiopulmonary arrest happens, ventilatory assist, cardiopulmonary resuscitation, and full resuscitation doses of atropine and epinephrine must be administered directly. The incidence of low-frequency hearing loss following dural puncture may be as high as 50%. It seems to be because of cerebrospinal fluid leak and, if persistent, may be relieved with an epidural blood patch. Hearing loss following common anesthesia can be due to a selection of causes and is much less predictable. Mechanisms embody middle ear barotrauma, vascular injury, and ototoxicity of medicine (aminoglycosides, loop diuretics, nonsteroidal antiinflammatory medicine, and antineoplastic agents). Moreover, the allergen will be the substance itself, a metabolite, or a breakdown product. Patients could additionally be uncovered to antigens through the respiratory tract, gastrointestinal tract, eyes, skin and from earlier intravenous, intramuscular, or peritoneal publicity. Anaphylaxis happens when inflammatory brokers are released from basophils and mast cells because of an antigen interacting with immunoglobulin (Ig) E. Direct activation of complement and IgG-mediated complement activation may find yourself in similar inflammatory mediator launch and activity. Depending on the antigen and the immune system components concerned, hypersensitivity reactions are classically divided into 4 sorts (Table 54�5). In many cases, an allergen (eg, latex) could trigger more than one sort of hypersensitivity response. Type I reactions contain antigens that cross-link IgE antibodies, triggering the release of inflammatory mediators from mast cells. The activated neutrophils trigger tissue injury by releasing lysosomal enzymes and toxic products. The Fc portion of these antibodies then associates with excessive affinity receptors on the cell surface of tissue mast cells and circulating basophils. During subsequent reexposure to the antigen, it binds the Fab portion of adjoining IgE antibodies on the mast cell surface, inducing degranulation and launch of inflammatory lipid mediators and additional cytokines from the mast cell. An elevated tryptase focus in the setting of scientific signs of hypersensitivity signals mast cell activation and is the diagnostic test of alternative for anaphylactic reactions. The mixed effects of those mediators can produce arteriolar vasodilation, increased vascular permeability, elevated mucus secretion, easy muscle contraction, and different medical manifestations of kind I reactions. When angioedema is intensive, it can be associated with giant fluid shifts; when it entails the pharyngeal or laryngeal mucosa, it could possibly quickly compromise the airway. Angioedema can lead to airway compromise and is frequently the cause for anesthesiology airway administration consultation within the emergency department. Angioedema is secondary to elevated capillary permeability secondary either to activation of mast cells or through kinin mediation. The bradykinin receptor antagonist icatibant can likewise be administered if out there.
Cheap myambutol 600 mg with amex
Patients with extreme continual lung illness might rely upon accessory muscles of respiration (intercostal and abdominal muscles) to actively encourage or exhale. Similarly, efficient coughing and clearing of secretions require these muscles for expiration. For these reasons, neuraxial blocks ought to be used with warning in patients with restricted respiratory reserve. Neuraxial anesthesia at the lumbar and sacral levels blocks both sympathetic and parasympathetic management of bladder operate. Loss of autonomic bladder management results in urinary retention till the block wears off. Patients with urinary retention ought to be checked for bladder distention after neuraxial anesthesia. This systemic response includes increased concentrations of adrenocorticotropic hormone, cortisol, epinephrine, norepinephrine, and vasopressin levels, as properly as activation of the renin�angiotensin�aldosterone system. Clinical manifestations embrace intraoperative and postoperative hypertension, tachycardia, hyperglycemia, protein catabolism, suppressed immune responses, and altered renal function. Neuraxial blockade can partially suppress (during main invasive stomach or thoracic surgery) or totally block (during lower extremity surgery) the neuroendocrine stress response. To maximize this blunting of the neuroendocrine stress response, neuraxial block ought to precede incision and continue postoperatively. Contraindications 9 Major contraindications to neuraxial anesthe- Clinical Considerations Common to Spinal & Epidural Blocks Indications Neuraxial blocks could also be used alone or in conjunction with common anesthesia for so much of procedures below the neck. As a major anesthetic, neuraxial blocks have proved most helpful in decrease belly, inguinal, urogenital, rectal, and lower extremity surgery. Upper stomach procedures (eg, gastrectomy) have been carried out with spinal or epidural anesthesia, however because it could be troublesome to safely obtain a sensory degree adequate for patient comfort, these strategies are less commonly used. If a neuraxial anesthetic is being thought of, the dangers and advantages must be discussed with the patient, and informed consent ought to be obtained. The affected person should be mentally ready for neuraxial anesthesia, and neuraxial anesthesia must be acceptable for the sort of surgery. Procedures that require maneuvers that might compromise respiratory perform (eg, pneumoperitoneum or pneumothorax) or these operations which are sia embrace lack of consent, coagulation abnormalities, severe hypovolemia, elevated intracranial strain (particularly with an intracranial mass), and an infection at the site of injection. Inspection and palpation of the back can reveal surgical scars, scoliosis, pores and skin lesions, and whether or not or not the spinous processes could be identified. Neuraxial anesthesia within the presence of sepsis or bacteremia may theoretically predispose sufferers to hematogenous spread of the infectious brokers into the epidural or subarachnoid area. Patients with preexisting neurological deficits or demyelinating ailments might report worsening symptoms following a neuraxial block. It could additionally be impossible to discern results or complications of the block from preexisting deficits or unrelated exacerbation of preexisting illness. For these reasons, some riskaverse practitioners argue in opposition to neuraxial anesthesia in such patients. In a retrospective examine examining the data of 567 sufferers with preexisting neuropathies, 2 of the patients developed new or worsening neuropathy following neuraxial anesthesia. Although this discovering signifies a comparatively low threat of further damage, examine investigators suggest that an injured nerve is vulnerable to additional harm, increasing the probability of poor neurological outcomes. However, a historical past of preexisting neurological deficits or demyelinating disease is at finest a relative contraindication, and the balance of perioperative risks in this patient inhabitants might favor neuraxial anesthesia in certain select patients. This may be difficult or inconceivable for patients with dementia, psychosis, or emotional instability. Unsedated younger kids will not be suitable for pure regional techniques; nonetheless, regional anesthesia is frequently used with general anesthesia in youngsters. Fortunately, the incidence of epidural hematoma is reported to be infrequent (1 in one hundred fifty,000 epidurals). The use of anticoagulant and antiplatelet medications continues to enhance, putting an ever-larger number of patients at potential threat of epidural hematomas.