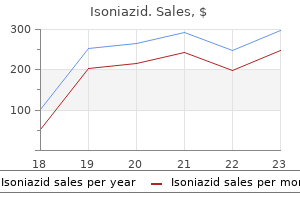
Isoniazid dosages: 300 mg
Isoniazid packs: 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

Isoniazid 300mg sale
An exception to these statements is the coma that arises from seizures, in which metabolism and blood flow are significantly elevated. Some of these metabolic modifications are probably epiphe nomena, reflecting in every specific encephalopathy a specific type of dysfunction in neurons and their support ing cells. Again, for many metabolic alterations, the rate of change is equivalently necessary to absolutely the level in causing a change in consciousness. Lactic acidosis might affect the brain by lowering arterial blood pH to lower than Yet one other unique type of coma is that produced by inhalation anesthetics. The effects of common anesthesia had for many years been attributed to adjustments within the phys ical chemistry of neuronal membranes. Inhalation anesthet ics are uncommon amongst coma-producing medication in respect to the sequence of inhibitory and excitatory results that they produce at different concentrations. During anes thesia, adequate inhibition of brainstem activity can be attained to remove the pupillary responses and the corneal reflex. Sustained clonus, exaggerated tendon reflexes, and Babinski signs are frequent in the course of the process of arousal. Preexisting focal cerebral deficits from strokes often worsen transiently with the administration of anesthetics, as is true to a lesser extent with different sedatives, metabolic encephalopathies, and hyperthermia. The impairment of consciousness that accompanies pulmo nary insufficiency is related mainly to hypercapnia. This is not to say that the toxic effects of those molecules has been confirmed or is nicely understood, as famous below. In acute hyponatremia (Na <120 mEq/L) of whatever cause, neuronal dysfunction is probably a results of the intracel lular movement of water, leading to neuronal swelling and loss of potassium chloride from the cells. Others, similar to methyl alcohol and ethylene glycol, each act instantly and by pro ducing a metabolic acidosis. Although the coma of poisonous and metabolic illnesses normally evolves via phases of drowsiness, confusion, and stupor (and the reverse sequence occurs throughout emergence from coma), each dis ease imparts its personal characteristic medical options. The sudden and extreme neuronal discharge that characterizes an epileptic seizure is one other widespread mechanism of coma. Coma then ensues, presumably because the extension of the seizure discharge to deep central neuronal structures paralyzes their perform. In other forms of seizures, during which consciousness is interrupted from the very begin ning, a diencephalic origin has been postulated (centren cephalic seizures of Penfield, as discussed in Chap. In closed head injury, it has been proven that in the intervening time of the concussive injury there is a gigantic increase in intracranial pres positive, on the order of 200 to seven hundred lb / in2, lasting a number of thou sandths of a second. The vibration set up in the cranium and transmitted to the mind was for a couple of years thought to be the idea of the abrupt paralysis of nervous function that characterizes concussive head damage (commotio cerebri). Disruption of the perform of neurons in some unknown method from the mechanical deformation is the proximate cause of loss of consciousness. These same bodily forces, when extreme, cause a number of shearing lesions or hemorrhages within the diencephalon and upper brainstem. A similar condition of periodic hyperarnm onemic coma in kids and adults can come about from urea cycle enzyme defects, such as orni thine transcarbamylase deficiency. Under the title of idiopathic recurring stupor, a uncommon situation has been described in grownup males who displayed a chronic state of deep sleepiness final ing from hours to days intermittently over a period of a few years. During the bouts, a 1 00 fold enhance of circulating endozepine-4, an ostensibly naturally occurring diazepine agonist, was present within the serum and spinal fluid. Subsequently; the authors of the unique reviews (Lugaresi et al) discovered, by the use of more superior strategies, that intoxication with lorazepam might have accounted for no less than a few of the cases. The vigilance-producing drug, modafinil, has additionally been efficient in a single report (Scott and Ahmed). A peculiar type of transient unresponsiveness in elderly people has been identified by Haimovic and Beresford. Our patients had no systemic sickness with this dysfunction and have been men of their eighth decade who lacked Babinski signs, pupillary abnormalities and, for essentially the most part, eye movement limitations (one had dis proportionately better horizontal than vertical gaze with oculocephalic testing). Patients with advanced Parkinson disease will occasionally show episodic unresponsive ness with eyes open. It is unclear to us whether migraine can cause a simi lar syndrome, as suggested within the research of familial hemi plegic migraine by Fitzsimmons and Wolfenden. Catatonic stupor and Kleine-Levin syndrome of periodic hypersomnolence and behavioral changes (Chap. The second is metabolic or submicroscopic, resulting in suppression of neuronal exercise in the cerebrum and reticular activating system.
Order isoniazid 300 mg on-line
The follow of surgical sectioning of the corpus callosum for the management of epilepsy greatly stimulated curiosity in the special capabilities of the best cerebral hemisphere when isolated from the left. It is within the sphere of visuospatial notion that right hemispheral dominance is most convincing. Lesions of the right posterior cerebral area result in an lack of ability to uti lize information about spatial relationships in making perceptual j udgments and in responding to objects in a spatial framework. This is manifest in developing When the entire corpus callosum is destroyed by tumor or surgical section, the language and notion areas of the left hemisphere are isolated from the best hemisphere. Patients with such lesions, if blindfolded, are unable to match an object held in a single hand with that within the different. In most lesions confined to the posterior portion of the corpus callosum (splenium), solely the visual a part of the disconnection syndrome occurs. Cases of occlu sion of the left posterior cerebral artery provide one of the best examples. Because infarction of the left occipital lobe causes a right homonymous hemianopia, all visual infor mation wanted for activating the speech areas of the left hemisphere must thereafter come from the best occipital lobe. There is, nevertheless, no issue in copying phrases; presumably, the visual information for activating the left motor space crosses the corpus cal losum extra anteriorly. Spontaneous writing and writing to dictation are also intact as a result of the language areas, including the angular gyrus, Wernicke and Broca areas, however after a delay, the affected person is unable to learn what he the syndrome of alexia has beforehand written (unless it was memorized). This is and the left motor cortex, are intact and interconnected, paraphasic speech and writing and comparatively intact comprehension of spoken and written language. The Wernicke area in the temporal lobe is putatively sepa rated from the Broca area, presumably by a lesion within the arcuate fasciculus or exterior capsule or subcorti cal white matter. However, most often the lesion is in the supramarginal gyrus, as mentioned in Chap. By destroying the origin of the fibers that connect the left and right motor association cortices, a lesion within the more ante rior components of the corpus callosum or the subcortical white matter underlying Broca space and contigu ous frontal cortex causes an apraxia of commanded actions of the left hand (see Chap. This defect has been attrib uted to a subcortical lesion of the left temporal lobe, spanning the Wernicke area and interrupting additionally these auditory fibers that cross within the corpus callo sum from the other aspect. Object naming and matching of colours without naming them are additionally done without error. Of interest to the authors is the fact that one some times encounters sufferers with a lesion in all or some a half of the corpus callosum with out with the power to dem onstrate any side of the aforementioned disconnec tion syndromes. Notable is the remark that in some sufferers with a congenital agenesis of the corpus callosum (a developmental abnormality), none of the interhemi spheral disconnection syndromes could be discovered. One should suppose that in such patients, information is transferred by one other route-perhaps the anterior or posterior com missure-or that dual dominance for language and praxis was established throughout early development. Furthermore, all the syndromes that span the occipital and either parietal or temporal lobes are, in impact intrahemispheral disconnections in the stream of visual data as mentioned earlier. The first consists of the statement and recording of qualitative modifications in habits and per formance and the identification of syndromes from which one may deduce the locus and nature of sure illnesses. An example is the deterioration index, deduced from the difference in performance on subtest objects of the Wechsler Adult Intelligence Scale that hold up well in cerebral diseases (vocabulary, information, image completion, and object assembly) and those that undergo impairment (digit span, similarities, digit symbol, and block design). A criticism of this index and others is the implicit assumption that cerebrocortical activity is a unitary function. In addition to the Wechsler alexia without agraphia, the next intrahemispheral disconnections have received essentially the most consideration. They are talked about here solely briefly and are thought of in more element within the following chapter. Milan Sorting Test, Halstead Category Test, and Wisconsin Card-Sorting Test as checks of capacity to summary and shift paradigms B. Environmental tory notion Sounds Test, and Austin Meaningless Sounds Test as measures of audi Parietal lobe issues A. Seashore Rhythm Test, Speech-Sound Per ception Test from the Halstead-Reitan battery, Occipital lobe disorders A.
Order cheapest isoniazid and isoniazid
Some sufferers, on the stage when the headache would have been prone to start, could faint, and others turn into confused or stuporous, a state that will persist for several hours or longer. The signs carefully resemble these attributable to ischemia in the terri tory of the basilar-posterior cerebral arteries-hence the name basilar artery or vertebrobasilar migraine. The headache could also be exceptionally extreme and abrupt in onset ("crash migraine" or "thunderclap headache"), elevating the specter of subarachnoid hemorrhage. A transient third-nerve palsy with ptosis, with or without involvement of the pupil, is the usual image; hardly ever, the sixth nerve is affected. The ocular paresis typically outlasts the headache by days or weeks; after many attacks, a slight mydriasis and, hardly ever, ophthalmoparesis could remain permanently. In some circumstances of uniocular visible disturbance with scotoma, the retinal arterioles have been reported to be attenuated and, not often, there are retinal hemorrhages as described by Berger and colleagues. Such occasions are referred to as retinal migraine, or, more accurately, ocular migraine, as either the retinal or the ciliary circulation could also be concerned. However, in adults the syndrome of headache, unilateral ophthalmoparesis, and loss of imaginative and prescient could have extra critical causes, including temporal (cranial) arteritis. Although typically hemicranial (the which, in flip, is from the Latin hemicrania, and its cor rupted forms hemigranea and migranea), the ache may be migraine is alleged to be derived from megrim, frontal, temporal, or, quite often, generalized. Any two of the three principal components-neuro logic abnormality, headache, and gastrointestinal upset could also be absent. One frequent configuration is a full-blown visual aura with out subsequent head ache (migraine with out headache, or migraine dissocie). A particularly troublesome migraine variant occurs in a child or adolescent who, after a trivial or delicate head damage, may lose vision, suffer severe headache or be plunged into a state of confusion, with belligerent and irrational behavior that lasts for hours or a quantity of days earlier than clearing. Although a family history of migraine is frequent in such cases, there has been no history of hemiplegia in other relations. Recurrent assaults have been referred to prior to now by pediatricians as the "periodic syndrome. Also, there are puzzling patients with bouts of fever or transient disturbances in mood ("psychic equivalents") and belly ache (abdominal migraine), that had been attributed to migraine however are doubtful entities at best. Recovery was complete, and arteriography in one youngster, after greater than 70 assaults, was normal. The relation ship of this condition to familial hemiplegic migraine (see below) stays unsure. The only benefit of consid ering such attacks as migrainous is that it could shield some sufferers from unnecessary diagnostic procedures and surgical intervention; however, by the same token, it may delay appropriate investigation and treatment. Rarely, migrainous neurologic signs, as a substitute of being transitory, leave a chronic or even everlasting deficit. This has been known as complicated migraine and a small number of these show to be migrainous infarc tions. Platelet aggregation, edema of the arterial wall, increased coagulability, dehydration from vomiting, and intense, extended spasms of vessels have all been impli cated (on quite uncertain grounds) within the pathogenesis of arterial occlusion and strokes that complicate migraine (Rascol et al). At the Mayo Clinic, in a gaggle of ages had 4,874 patients 50 years or youthful with a analysis of migraine, migraine equal, or vascular headache, 20 patients migraine-associated infarctions (Broderick and Swanson). Several families have been described by which this situation is the end result of a mutation in an ion of migraine have been sophisticated by strokes in the verte brobasilar territory. A more recent examine by Wolf and colleagues collected 17 cases of stroke and migraine. Most had a chronic aura, both visible, sensory or aphasic and over two-thirds of the strokes, demonstrated by diffusion restriction on (familial hemiplegic migraine; alternating hemiplegia of childhood). There is, nonetheless, a paucity of useful pathology by which to interpret the mechanism of migraine-associated stroke. The unsure however potential position of antimigraine medica tions in producing stroke is mentioned further on within the part on remedy. Estrogen drugs have additionally been implicated in stroke in some girls migraineurs.
Order discount isoniazid line
Numerous monographs and articles have been written in regards to the signal: a fairly comprehensive one, by van Gijn, and an elegant however extra arcane one by Fulton and Keller. In its essential type, the sign consists of extension of the large toe and extension and fanning of the opposite toes throughout and immediately after stroking the lateral plantar floor of the foot. The stimulus is applied along the dorsum of the foot from the lateral heel and sweeping upward and across the ball of the foot. Several dozen surrogate responses (with numer ous eponyms) have been described over the years, most utilizing alternative sites and kinds of stimulation, however all have the identical significance as the Babinski response. Clinical and electrophysiologic observations indicate that the extension motion of the toe is a element of a larger synergistic flexion or shortening reflex of the leg-i. The most characteristic of these is the "tri ple flexion response", by which the hip, thigh and ankle flex (dorsiflex) slowly, following an appropriate stimulus. These spinal flexion reflexes, of which the Babinski sign is the most characteristic, are frequent accompaniments to-but not important components of-spasticity. They are current due to disinhibition or launch of motor packages of spinal origin. Important traits of these responses are their capacity to be induced by weak superficial stimuli (such as a sequence of pinpricks) and their tendency to persist for a few moments after the stimula tion ceases. With incomplete suprasegmental lesions, the response may be fractionated; for instance, the hip and knee might flex but the foot may not dorsiflex, or vice versa. The hyperreflexic state that characterizes spasticity could take the type of clonus, a sequence of rhythmic involun tary muscular contractions occurring at a frequency of 5 to 7 Hz in response to an abruptly utilized and sustained stretch stimulus. It is often designated in phrases of the a half of the limb to which the stimulus is applied. Clonus requires an appro priate degree of muscle rest, integrity of the spinal stretch reflex mechanisms, sustained hyperexcitability of alpha and gamma motor neurons (suprasegmental effects), and synchronization of the contraction-relaxation cycle of muscle spindles. The cutaneomuscular stomach and cremasteric reflexes ("cutaneous, or superficial reflexes") are elicited by speedy, mild stroking of the pores and skin overlying these muscle tissue, and are often abolished when the upper motor neuron is damaged. These were referred to as reflexes earlier than the tip of the nineteenth century, which leads to some confusion in deciphering the older clinical literature. Spread, or radiation of reflexes, is regularly related to spasticity, although the latter phenomenon may be noticed to a slight degree in regular persons with brisk tendon reflexes. Tapping of the radial periosteum, for example, could elicit a reflex contraction not solely of the brachioradialis but additionally of the biceps, triceps, or finger flexors. This spread of reflex activity is probably not the result of radiation of impulses within the spinal twine, but a result of the propagation of a vibration wave from bone to muscle, stimulating the excitable muscle spindles in its path (Lance). Other manifestations of the hyperreflexic state, are the Hoffmann signal and the crossed adduc tor reflex of the thigh muscle tissue. Also, reflexes could also be "inverted," as within the case of a lesion of the fifth or sixth cervical section; here the biceps and brachioradialis reflexes are abolished and solely the triceps and finger flexors, whose reflex arcs are intact, respond to a tap over the distal radius. With bilateral cerebral lesions, exaggerated stretch reflexes may be elicited in cranial as properly as limb and trunk muscle tissue due to interruption of the corticobul bar pathways. These are seen as easily triggered masseter contractions in response to a brisk downward faucet on the chin ("jaw jerk") and brisk contractions of the orbi cularis oris muscular tissues in response to tapping the philtrum or corners of the mouth. In advanced circumstances, weak point or paralysis or slowness of voluntary movements of the face, tongue, larynx, and pharynx are added (bulbar spas ticity or "pseudobulbar" palsy; see additionally Chap. The many investigations of the biochemical changes that underlie spasticity and the mechanisms of action of antispasticity drugs have been reviewed by Davidoff. Because glutamic acid is the neurotransmitter of the corti cospinal tracts, one would count on its action on inhibitory interneurons to be lost. Actually, none of those brokers is entirely satisfactory within the remedy of spasticity when administered orally; the administration of baclofen intra thecally at instances has a extra useful effect. Glycine is the transmitter released by inhibitory interneurons and is measurably decreased in quantity, uptake, and turnover in the spastic animal. There is a few proof that the oral administration of glycine reduces experimentally induced spasticity, however its value in patients is uncertain. Interruption of descending noradrenergic, dopaminergic, and serotonergic fibers is undoubtedly involved within the genesis of spasticity, though the exact mode of motion of those neurotransmitters on the various parts of spinal reflex arcs remains to be outlined.
Order cheap isoniazid line
If such contractions happen singly or are repeated in a restricted group of muscle tissue, such as these of an arm or leg, the phe nomenon is termed segmental myoclonus, whereas extensive unfold, lightning-like, arrhythmic repeated contractions are referred to as polymyoclonus. The dialogue that fol lows makes evident that every of the three phenomena has a particular pathophysiology and clinical implications. It is most easily elicited by forcefully dorsiflexing the ankle; a sequence of rhythmic jerks of small to reasonable amplitude end result. A widespread and benign example of myoclonus, famil iar to many persons, is the "sleep-start" that consists of a jerking of the body, significantly the torso, whereas falling asleep or occasionally, simply previous to waking (see Chap. This movement shall be vigorous sufficient to trigger tongue biting and be mistaken for a convulsion. Epilepsia partialis continua is a particular sort of rhyth mic epileptic exercise during which one group of muscle tissue often of the face, arm, or leg-is continuously (day and night) involved in a collection of rhythmic monophasic con tractions. It consists of arrhythmic lapses of sustained posture that enable gravity or the inherent elasticity of muscle tissue to produce a motion, which the patient then corrects, sometimes with overshoot. This confirmed that asterixis differs physi ologically from each tremor and myoclonus, with which it was formerly confused; it has incorrectly been referred to as a "adverse tremor. Flexion actions of the hands may then occur arrhythmically as quickly as or several occasions a minute. The same lapses in sus tained muscle contraction could be provoked in any muscle group-including, for example, the protruded tongue, the closed eyelids, or the flexed trunk muscle tissue. Sometimes, asterixis can be elicited best by asking the patient to place his hand flat on a table and lift the index finger. This sign was first noticed in patients with hepatic encephalopathy but was later noted with hypercapnia, uremia, and different metabolic and poisonous encephalopathies. Asterixis may also be evoked by phenytoin and other anticonvulsants, often indicating that these drugs are current in extreme concentrations. Similar rapid lapsing movements of the head or arms generally seem dur ing drowsiness in normal persons ("nodding off"). Unilateral asterixis happens in an arm and leg on the facet opposite an anterior thalamic infarction or small hemorrhage, after stereotaxic thalamotomy; and with an upper midbrain lesion, often as a transient phenom enon after stroke. One-sided or focal myoclonic jerks are the dominant feature of a selected form of childhood epilepsy-so-called benign epilepsy with rolandic spikes (Chap. Myoclonus could also be associated with atypi cal petit mal and akinetic seizures within the Lennox-Gastaut syndrome (absence or petit mal variants); the affected person typically falls through the brief lapse of postural mechanisms that follows a single myoclonic contraction. These forms of special "myoclonic epilepsies" are discussed further below and in Chap. As a outcome, an arm might abruptly flex, the head could jerk backward or ahead, or the trunk might curve or straighten. In this and other types of myoclonus, the muscle contraction is brief (20 to 50 ms)-i. The speed of the myoclonic contraction is similar whether or not it involves part of a muscle, a complete muscle, or a group of muscles. Some of the patients register little grievance, accept ing the fixed intrusions of motor activity with sto icism; they generally lead comparatively regular, active lives. Adams, essential tremor was current as well, both in family mem bers with polymyoclonus and in these without. Both the tremor and myoclonus had been dramatically suppressed by the ingestion of alcohol. In a Mayo Clinic collection reported by Aigner and Mulder, 19 of ninety four instances of polymyoclonus had been of this "important" sort. Several of the sleep-related syndromes that involve repetitive leg movements include an element of myoc lonus. In a few patients, primarily older ones with extreme "restless legs syndrome," the myoclonus and dyskinesias could turn out to be troublesome in the daytime as properly. It was most likely in the course of this description that the term myoclonus was used for the primary time. Muscles were concerned diffusely, significantly these of the decrease face and proximal segments of the limbs, and the myoclonus continued for a quantity of years, being absent solely throughout sleep.
Purchase isoniazid 300 mg
In approximately 70 percent of all sufferers with epi lepsy; the seizures are managed fully or virtually utterly by drugs; in an extra 20 to 25 per cent, the assaults are significantly decreased in number and severity. Table 16-5 lists the most generally used medicine together with their dosages, effective blood levels, and serum half-lives. Because of the lengthy half-lives of phenytoin, phe nobarbital, and ethosuximide, these medication want be taken only once daily, preferably at bedtime. Valproate and carba mazepine have shorter half-lives, and their administration should be spaced in the course of the day. It is helpful to be familiar with the serum protein-binding characteristics of antiepi leptic medicine and the interactions amongst these medicine, and between antiepileptic and different medicine. Initially, just one drug must be used and the dosage elevated until sustained therapeutic lev els have been attained. A general method to the selection of drug in sure frequent types of epilepsy is given in Tables 16-6 for adults and 1 6-7 for kids, however it have to be noted that there are a number of medicine that could be appropriate in each circumstance. It is troublesome to give definitive steerage on combin ing medications for refractory seizures. Second, the clinician ought to be aware of identified interactions by way of metabolic pathways such as valpro ate combined with either lamotrigine or phenobarbital as they share the cytochrome P450 degradation pathway. The therapeutic dose for any given affected person should be decided, to some extent by medical impact, guided by measurement of serum levels, as described beneath. Inquiry concerning seizure control and drug side effects is extra priceless than adjustment of medica tion based mostly solely on drug concentrations. Not uncommonly, a drug is discarded as being ineffective when a slight improve in dosage would have led to suppression of assaults. On the opposite hand, drug levels could be useful in detecting non-compliance or poor absorption in situations of inadequate seizure management. The administration of seizures is facilitated by having sufferers chart their every day medication and the number, time, and circumstances of each episode. This indi cates to the affected person whether or not a dose had been missed and whether the supply of medications is operating low. Table 16-5 signifies the efficient serum levels for each of the commonly used antiepileptic medication. The scenario may be further compli cated by interactions between one anticonvulsant and the metabolites of another, as, for example, the inhibi tion of epoxide hydrolase by valproic acid, leading to toxicity through the buildup of carbamazepine epoxide. In circumstances of unexplained toxicity in the face of conventionally obtained serum ranges which might be regular, measurement could also be undertaken of the levels of free drug and the focus of active metabolites by chro matographic strategies. The use of saliva for measurement of free drug levels has advantage but has not been adopted incessantly in follow. It has the benefit of permitting the affected person to gather a sample earlier than breakfast and keep away from venipuncture. This is especially true of phenytoin, which, as the outcomes of saturation of liver enzy matic capability, has nonlinear kinetics once serum con centration exceeds 10 mg/mL. For this purpose, a typical improve in dose from 300 to 400 mg day by day results in a dis proportionate elevation of the serum level and toxic unwanted effects. Elevations in drug concentrations are also accom panied by prolongation of the serum half-life, which will increase the time to reach a steady-state focus of phenytoin after dosage changes. Contrariwise, carba mazepine is thought to induce its own metabolism, in order that doses adequate to management seizures at the outset of therapy are no longer effective a quantity of weeks later. Although many such interactions are known, just a few are of medical significance and most pertain to older generations of medications, requiring adjustment of drug dosages (see Kutt). Among interactions between anticonvulsant medicine, valproate often results in accumulation of active phenytoin and of phenobarbital by displacing them from serum proteins, as properly as barely elevating serum whole ranges. Agents that alter the concentrations of anti epileptic medications are chloramphenicol, which causes the buildup of phenytoin and phenobarbital, and erythromycin, which causes the accumulation of carba mazepine. Antacids cut back the blood phenytoin con centration, whereas histamine blockers used to reduce gastric acid output do the other. Salicylates reduce the whole plasma ranges of anticonvulsant medicine however elevate the free fraction by displacing the drug from its protein carrier. Enzyme-inducing drugs such as phenytoin, carbamaze pine, and barbiturates can significantly enhance the chance of breakthrough menstrual bleeding in ladies taking oral contraceptives and will result in failure of contraceptive medicines, and adjustments in the quantity of estradiol must be made. These interactions are emphasised additional below beneath the discussions of every agent. Hepatic perform greatly impacts antiepileptic drug concentrations, since most of those medicine are metabo lized in the liver.
Order isoniazid in india
Lesions confined to the motor cortex are reported to assume the form of clonic contractions, and those confined to the premotor cortex (area 6), tonic contractions of the contralateral arm, face, neck, or all of 1 facet of the body. Tonic elevation and extension of the contralateral arm ("fencing posture") and choreoathetotic and dystonic postures have been related to excessive medial frontal lesions (area 8 and supplementary motor cortex), as have advanced, weird, and flailing actions of a contralateral limb, but this at all times raises the suspi cion of hysterical seizure. Perspiration and piloerection occur occasionally in parts of the physique involved in a focal motor seizure, suggesting that these autonomic func tions have a cortical representation in or adjoining to the rolandic space. Focal motor and Jacksonian seizures have primarily the same localizing significance. Seizure discharges arising from the cortical language areas may give rise to a short aphasic disturbance (ictal aphasia) and ejaculation of a word or, more incessantly, a vocal arrest. Ictal aphasia is normally succeeded by other focal or generalized seizure activity but could occur in iso lation, without loss of consciousness, by which case it could later be described by the patient. Postictal aphasia is extra common than ictal aphasia, which generally takes the form of complete speech arrest. Verbalization on the onset of a seizure has no constant lateralizing significance and, paradoxically, is normally related to an origin within the nondominant hemisphere. These disturbances should be distinguished from the stereotyped repetition of phrases or phrases or the garbled speech that characterizes some advanced partial seizures or the postictal confusional state and, in fact, Wernicke aphasia. Penfield and Kristiansen discovered the seizure focus in the postcentral or precentral convolution in 49 of fifty five such instances. The sensory disorder is usually described as numbness, tingling, or a "pins and-needles" feeling and sometimes as a sensation of crawling (formication), electrical energy, or movement of the part. In the overwhelming majority of cases, the onset of the sensory seizure is within the lips, fingers, or toes, and the spread to adjacent elements of the body follows a pattern determined by sensory preparations within the postcentral (postrolandic) convolution of the parietal lobe. If the sensory symptoms are localized to the head, the major focus is in or adjacent to the bottom a part of the convolution, close to the sylvian fissure; if the symptoms are in the leg or foot, the upper a half of the convolution, close to the superior sagittal sinus or on the medial floor of the hemisphere, is concerned. Gustaton; hallucinations even have been recorded in proven instances of temporal lobe illness and fewer often with lesions of the insula and parietal operculum; salivation and a sen sation of thirst could additionally be related. Electrical stimulation in the depths of the sylvian fissure, extending into the insular area, has produced peculiar sensations of taste. Lesions in or close to the striate cortex of the occipital lobe usually produce elemental visible sen sations of darkness or sparks and flashes of sunshine, which can be stationary or transferring and colorless or colored. According to Cowers, red is probably the most regularly reported shade, followed by blue, green, and yellow. These pictures may be referred to the visible field on the aspect opposite of the lesion or may appear straight forward. Curiously, a seizure arising in one occipital lobe might cause momentary blind ness in each fields. It has been noted that lesions on the lateral floor of the occipital lobe (Brodmann areas 18 and 19) are likely to trigger a sensation of twinkling or pulsating lights. More complex or shaped visual hal lucinations are often caused by a spotlight in the pos terior part of the temporal lobe, close to its junction with the occipital lobe, and could also be related to auditory hallucinations. The localizing value of visual auras has been confirmed by Bien and colleagues in a gaggle of 20 surgically handled sufferers with intractable seizures. They found that elementary visible hallucinations and visible loss have been typical of occipital lobe epilepsy however might additionally happen with seizure foci in the anteromedial temporal and occipitotemporal areas. Auditory hallucinations are rare as an preliminary manifestation of a seizure and usually characterize a psy chotic dysfunction or one of a quantity of extra benign conditions. Occasionally; a affected person with a spotlight in a single superior tem poral convolution will report a buzzing or roaring in the ears. A human voice, generally repeating unrecognizable phrases, or the sound of music has been noted a number of times with lesions in the extra posterior part of one temporal lobe. Vertiginous sensations of a type suggesting a vestibu lar origin could on rare events be the primary symptom of a seizure. The lesion is often situated in the superopos terior temporal area or the junction between parietal and temporal lobes. In one of many cases reported by Penfield and Jasper, a sensation of vertigo was evoked by stimulating the cortex on the junction of the parietal and occipital lobes.
Buy discount isoniazid line
Other websites of tenderness and the buildings implicated by disease are proven within the determine. In palpating the spinous processes, it is necessary to note any deviation in the lateral aircraft (this may be indicative of fracture or arthritis) or in the anteroposterior plane. A "step-off" ahead displacement of the spinous process and exaggerated lordosis are necessary clues to the presence of spondylolisthesis (see additional on). Many of the processes discussed above can coexist, especially within the older individual, who may have hip and lumbar spine osteoarthropathy. This makes the interpre tation of assorted signs tough until the signs are first analyzed correctly. On completion of the examination of the again and legs, one turns to a search for motor, reflex, and sensory adjustments within the decrease extremities (see "Herniation of Lumbar Intervertebral Discs," additional on on this chapter). Region of sacrosciatic notch (tenderness = fourth or fifth lumbar rlisc rupture and sacroiliac sprain). Radiographs of the lumbar backbone may be helpful within the routine evaluation of low again ache and sciatica and may be carried out with the affected person in flexed and extended positions in the anteroposterior, lateral, and oblique planes. Readily demonstrable in plain films are narrowing of the intervertebral disc spaces, bony facetal or vertebral overgrowth, displacement of vertebral our bodies (spondy lolisthesis), and an unsuspected infiltration of bone by cancer. This results in an anterior displacement of 1 vertebral physique in relation to the adjoining one, spondylolisthesis. The primary explanation for spondylolisthesis in older adults is degenerative arthritic disease of the spine as mentioned additional on. Patients with progressive vertebral displace ment and neurologic deficits require surgery. Reduction of displaced vertebral bodies before fusion and direct repair of pars defects are possible in special circumstances. A common anomaly is fusion of the fifth lumbar vertebral physique to the sacrum ("sacralization") or, con versely, separation of the primary sacral section, giving rise to 6, somewhat than the usual 5 lumbar vertebrae ("lum barization"). However, neither of these is consistently related to any type of again derangement. Another one or a quantity of of the lumbar vertebrae or of the sacrum less-common finding is a lack of fusion of the laminae of (spina bifida). The anomaly could additionally be accompanied by malformation of vertebral joints and usually induces pain solely when aggravated by injury. The neurologic features of defective fusion of the backbone (dysraphism) are discussed in Chap. Many different congenital variants have an result on the lower lumbar vertebrae: asymmetrical aspect joints, abnormali ties of the transverse processes, are seen sometimes in patients with low again signs, however apparently with no larger frequency than in asymptomatic people. Spondylolysis consists of a congenital and doubtless genetic bony defect in the pars interarticularis (the section at the junction of pedicle and lamina) of the lower lumbar ver tebrae. In extreme acute accidents from direct impact the examiner should be careful to keep away from further harm and actions ought to be stored to a minimal until an approximate diagnosis has been made. Furthermore, what was previously referred to as "sacroiliac strain" or "sprain" is now known to be caused by, in some situations, disc illness. The term acute low again pressure may be preferable for minor, self-limiting accidents that are usu ally associated with lifting heavy masses when the again is in a mechanically deprived place, or there might have been a fall, prolonged uncomfortable postures corresponding to in air journey or automotive rides, or sudden unexpected movement, as could occur in an auto accident. Nonetheless, the discomfort of acute low again strain may be extreme, and the patient might assume unusual pos tures related to spasm of the decrease lumbar and sacrospi nalis muscular tissues. The pain is normally confined to the lower part of the again, in the midline, throughout the posterior waist, or just to one side of the backbone. The analysis of lumbo sacral strain depends on the biomechanics of the damage or exercise that precipitated the ache. The injured structures are recognized by the localization of the ache, the finding of localized tenderness, augmentation of pain by postural changes-e. In more than 80 p.c of circumstances of acute low again strain of this type, the ache resolves in a matter of several days or a week, even with no particular remedy. The defect assumes significance in that it predis poses to delicate fracture of the pars articularis, generally precipitated by slight trauma however usually in the absence of an appreciated harm. The ache of muscular and ligamentous strains is normally self-limiting, responding to simple measures in a comparatively brief time period. The basic precept of therapy in both disorders is to keep away from reinjury and cut back the discomfort of painful components.