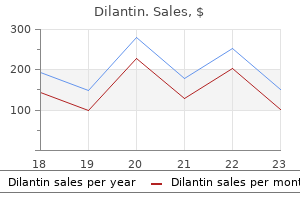
Dilantin dosages: 100 mg
Dilantin packs: 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

Purchase 100mg dilantin amex
D, Chronic inflammatory cell infiltrate with fibrosis corresponding to late part of illness. A, Multifocal lytic and sclerotic lesion involving each clavicles and third right rib. B, Radioisotopic bone scan of identical patient as proven in A shows multifocal increased uptake in right third rib and each clavicles. C, Diffuse lytic and sclerotic process with bone enlargement involving left clavicle (same affected person as in A and B). D, Chronic inflammatory infiltrate with predominance of lymphocytes and related fibrosis. B, T2-weighted magnetic resonance image exhibits excessive sign depth in central (cystic) portion of lesion. C, Pathologic fracture by way of tumor amyloidosis involving distal femoral finish in affected person with plasma cell dyscrasia and related disseminated amyloidosis. Amir G, Mogle P, Sucher E: Case report 729: myositis ossificans and aneurysmal bone cyst. Dahl I, Angervall L: Pseudosarcomatous lesions of the soft tissues reported as sarcoma throughout a 6-year period (1958-1963). Dahl I, Angervall L: Pseudosarcomatous proliferative lesions of soft tissue with or without bone formations. Kaleli T, Temiz A, Ozt�rk H: Pseudomalignant myositis ossificans of the wrist causing compression of the ulnar nerve and artery. Konishi E, Kusuzaki K, Murata H, et al: Extraskeletal osteosarcoma arising in myositis ossificans. Leithner A, Weinhaeusel A, Zeitlhofer P, et al: Evidence of a polyclonal nature of myositis ossificans. Povysil C, Matejovsky Z: Ultrastructural proof of myofibroblasts in pseudomalignant myositis ossificans. Sazbon L, Najenson T, Tartakovsky M, et al: Widespread periarticular new-bone formation in long-term comatose sufferers. Sumiyoshi K, Tsuneyoshi M, Enjoji M: Myositis ossificans: a clinicopathologic examine of 21 instances. Buyse G, Silberstein J, Goemans N, et al: Fibrodysplasia ossificans progressiva: still turning into wood after 300 years Ehara S, Nishida J, Abe M, et al: Magnetic resonance imaging of pseudomalignant osseous tumor of the hand. Endo M, Hasegawa T, Tashiro T, et al: Bizarre parosteal osteochondromatous proliferation with a t(1;17) translocation. Hirao K, Sugita T, Yasunaga Y, et al: Florid reactive periostitis of the metatarsal bone: a case report. Mertens F, Moller E, Mandahl N, et al: the t(X;6) in subungual exostotis leads to transciptional deregulation of the gene for insulin receptor substrate four. Suga H, Mukouda M: Subungual exostosis: a review of 16 cases focusing on postoperative deformity of the nail. Sundaram M, Wang L, Rotman M, et al: Florid reactive periostitis and weird parosteal osteochondromatous proliferation: prebiopsy imaging evolution, treatment and outcome. Miao J, Zhang C, Wu S, et al: Genetic abnormalities in fibrodysplasia ossificans progressiva. Thickman D, Bonakdar-pour A, Clancy M, et al: Fibrodysplasia ossificans progressiva. Dupuytren G: On the injuries and illnesses of bones, London, 1847, Publications of the Sysdenham Society (translated by F LeGros Clard). Yuen M, Friedman L, Orr W, et al: Proliferative periosteal processes of phalanges: a unitary hypothesis. Joerring S, Krogsgaard M, Wilbek H, et al: Collagen turnover after tibial fractures. Massey T, Garst J: Compartment syndrome of the thigh with osteogenesis imperfecta: a case report. Postacchini F, Gumina S, Perugia D, et al: Early fracture callus in the diaphysis of human lengthy bones: histologic and ultrastructural examine. Blumberg N, Arbel R, Dabby D: Avulsion of the triceps tendon throughout acceleration stress.
Diseases
- Blomstrand syndrome
- Chondrodysplasia punctata, brachytelephalangic
- Erythroblastopenia
- Lipoid congenital adrenal hyperplasia
- Staphylococcus epidermidis infection
- Glycogen storage disease type 1B
- Reinhardt Pfeiffer syndrome
- Forney Robinson Pascoe syndrome
Buy generic dilantin 100mg
If, after placing the primary finger, a second finger is needed to push the lid upward, spacer insertion is required within the decrease lid to achieve the vertical vector for upward movement. We normally omit using the third finger, as a result of pores and skin recruitment is accomplished with the primary finger. If the decrease lid resists upward movement because of stiffness resulting from adhesions within the lid or scarring towards the orbital rim, a firm spacer is required to forestall a recurrence of retraction. When positioning the spacer, one must consider the blood provide to the lower lid to forestall devitalizing the margin. The inferior arcade travels 4 mm beneath the decrease lid margin, and a major majority of blood flow to the decrease lid comes from the nasal side. A single finger is placed at the lateral canthus, and the decrease lid is pushed in an upward and outward vector. If lid repositioning occurs with one lateral finger pushing up, a lateral canthoplasty with out the need for a spacer can be used. If a second finger is needed in the midportion of the lid to obtain good decrease lid repositioning, a spacer is required and should be included as a part of the preoperative process. It is inserted in the eyelid via a partial- or full-thickness blepharotomy 6 mm below the eyelid margin. The partial-thickness blepharotomy is more generally used, is safer, and preserves the orbicularis in situ via an anterior strategy to make positive the blood provide to the lower lid margin. Release of the posterior lamellar scar via a canthotomy and posterior approach should launch the conjunctiva, capsulopalpebral fascia, and the posterior lamellar scar, holding the lid down whereas preserving the orbicularis. The spacer is inserted via an incision within the conjunctiva, with release of the capsulopalpebral fascia and posterior lamellar scar until the lid is vertically launched. If skin recruitment is needed, dissection of the cheek by way of the transconjunctival incision with launch of the orbitomalar ligament and either minimal preperiosteal dissection or more aggressive subperiosteal dissection may be performed to mobilize skin and orbicularis for recruiting pores and skin into the decrease lid to decrease anterior lamellar shortage. These patients are considered to be at excessive risk for lid malposition after decrease blepharoplasty regardless of lateral canthopexy and orbicularis redraping. Release of the orbitomalar ligament and recruitment of skin and muscle is completed both with preperiosteal dissection or posterior lamellar dissection. The lid is then elevated by launch of the scarred layer, which is often deep to the orbicularis, and a spacer graft is positioned through the transcutaneous or anterior strategy. This is at all times combined with a lateral canthoplasty and orbicularis suspension with a periosteal suture or a bony Mitek anchor. It is probable that further crosslinked collagen merchandise shall be launched into the medical market. When larger items are used (that is, higher than eight mm in vertical width), some protection with conjunctiva may velocity the reepithelialization process. With any spacer, significantly absorbable collagen spacers, a postoperative interval of elevated manufacturing of mucus and mild irritation occurs, which can be controlled with topical steroids. Occasional pyogenic granulomas occur with the use of any spacer; these are simply treated with easy excision in the office. The average quantity of spacer used is 6 mm in vertical width; nevertheless, the quantity of spacer inserted is the quantity judged to be essential intraoperatively. It is definitely not a 1:1 ratio of spacer-to-lid elevation, since extra spacer needs to be used than the amount of vertical elevation desired. No set formulation can be used preoperatively to decide the quantity, and the ultimate determination occurs during surgical procedure. B, In beforehand unoperated cases, spacer material is often positioned transcutaneously, as a result of most require external skin redraping and resection for aesthetic causes. C, She is proven after present process ear cartilage spacer insertion with canthal anchoring. The drawback of ear cartilage is its long-term visibility, which regularly necessitates native excision of the seen edges. C, She is proven after lower lid repositioning with a vertical vector midface lift and lateral canthal anchoring. In some sufferers with very outstanding eyes and extra excessive lower lid retraction, a wider vertical width of spacer (up to 1 cm in vertical width) may be needed. For these sufferers, a particular method is required to safe the spacer in place; this includes placing transcutaneous quilting sutures to stabilize the upper edge of the spacer. We generally undermine the fornix conjunctiva to cover exposed spacer materials when wider spacers are used. D, Lid eversion reveals misalignment of the superior fringe of the spacer, ensuing from rigidity; trimming was required.
Cheap dilantin 100mg online
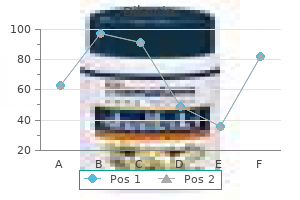
B, Regurgitation saline resolution injection showing flow back out from the higher canaliculus when the lower canaliculus is irrigated within the presence of distal nasolacrimal duct obstruction. Overprobing is a very common explanation for permanent canalicular scarring and blockage. Probing is used only as a diagnostic software in adults to determine the placement of a stricture in the canalicular system. The residual size of patency in the canaliculus could be decided in this method, and thus the absolute best corrective process for the affected person could be chosen. Ethmoidal sinus enlargement corresponding to ethmoidal mucocele or anterior encroachment of the ethmoidal sinus space could additionally be detected in addition to any erosion which could be attributable to a neoplastic process. This goal take a look at can be very useful in diagnosing or verifying lacrimal drainage insufficiency and is best performed with slitlamp examination. One drop of 2% sodium fluorescein is instilled in the lower conjunctival cul-de-sac. Zero represents no dye remaining, and 4+ indicates that virtually the entire dye remains. Normal patients may have a faint yellow fluorescein colour (for example, 1+) at the finish of 5 minutes. As said above, evaluating the two eyes is often extra significant than arduously trying to quantify and grade the results in one eye. Elderly sufferers with intermittent epiphora signs may not all the time have an sufficient precorneal tear movie. The dye disappearance take a look at is an easy, objective means of assessing lacrimal outflow function in these patients. It is clear that not all functional blockages are of the same severity, and more sophisticated tests are needed to quantitate the severity of a useful blockage. These checks are helpful primarily within the differential diagnosis of epiphora in patients with incomplete or useful blockage of the lacrimal sac or nasolacrimal duct. The precorneal tear movie is stained by instilling 2% fluorescein ophthalmic drops. The inferior turbinate in the ground of the nose laterally is then sprayed with decongestant and topical anesthetic. A dry cotton roll fluff, about one third the diameter of a cigarette, is wrapped around a nasal wire (or a straightened paper clip) and placed under the anterior half of the inferior turbinate (cotton-tipped applicator sticks are too massive to find sufficient placement underneath the turbinate). One can differentiate these, as well as estimate the extent of blockage, by the Jones secondary dye test. The punctum is anesthetized with a cotton-tipped applicator soaked in cocaine or tetracaine drops and then dilated with a punctal dilator. An irrigation cannula hooked up to a 3 ml syringe is inserted via the inferior punctum and canaliculus. The affected person is instructed to tip his or her head over a white porcelain basin so that any dye irrigated by way of the system shall be retrieved. This can be carried out as above or simply with Schirmer 1 with a filter paper strip and no tetracaine to measure the reflex lacrimation and Schirmer 2 with tetracaine to measure baseline tear manufacturing. The irrigation of fluid via the system with the appearance of dye (positive Jones 2) and no reflux of irrigant indicates a partial stenosis or a useful blockage. With a medial ectropion, one might not get well dye within the main dye test and but irrigate fluid via the nasolacrimal duct simply. Although the vast majority of tear drainage is by the inferior canaliculus, the upper canaliculus additionally supplies sufficient drainage for the traditional eye with out the contribution of the inferior canaliculus. The 30-minute dacryocystogram dye retention examine is helpful in confirming a nasolacrimal duct obstruction. In this test, water-soluble distinction dye is irrigated through the lacrimal outflow system. The presence of a significant amount of retained contrast dye within the lacrimal sac or nasolacrimal duct indicates a functional obstruction of the nasolacrimal duct. Radiopaque dye is injected forcibly into the lower canaliculus with a syringe using a lacrimal cannula or polyethylene tube. To keep away from obscuring particulars, dye ought to be wiped from the lids earlier than radiographs are taken. Dacryocystography may be useful to show the dimensions of the sac; the connection of the ethmoidal air cells to the lacrimal sac; filling defects within the sac, corresponding to lacrimal casts or lacrimal sac tumors; diverticula and fistulas of the sac; and presumably the precise stage of the stricture inside the lacrimal sac or nasolacrimal duct.
Cheap dilantin online visa
Campanacci M, Laus M, Boriani S: Multiple non-ossifying fibromata with extraskeletal anomalies: a brand new syndrome Charache H: Multiple neurofibroma with sarcomatous transformation and skeletal involvement. Chen S, Liu C, Liu B, et al: Schwannomatosis: a brand new member of neurofibromatosis family. Daimaru Y, Hashimoto H, Enjoji M: Malignant peripheral nerve sheath tumors (malignant schwannomas): an immunohistochemical research of 29 cases. Eisenbarth I, Hoffmeyer S, Kaufmann D, et al: Analysis of an alternatively spliced exon of the neurofibromatosis type I gene in cultured melanocytes from patients with neurofibromatosis 1. MacCollin M, Woodfin W, Kronn D, et al: Schwannomatosis: a scientific and pathologic research. Matsunou H, Shimoda T, Kakimoto S, et al: Histopathologic and immunohistochemical research of malignant tumors of peripheral nerve sheath (malignant schwannoma). Richard S, Gardie B, Couve S, et al: von Hippel-Lindau: How a uncommon illness illuminates most cancers biology. Skalova A, Sima R, Bohus P, et al: Endolymphatic sac tumor (aggressive papillary tumor of center ear and temporal bone). Tsuneyoshi M, Enjoji M: Primary malignant peripheral nerve tumors (malignant schwannomas): a clinicopathologic and electron microscopic study. Secondary cystic modifications in preexisting situations, corresponding to in chondroblastoma, fibrous dysplasia, and giant-cell tumor, are mentioned at the facet of these underlying circumstances. The growth of secondary aneurysmal bone cyst engrafted on different lesions is also mentioned in this chapter. Aneurysmal bone cyst is a multiloculated cystic lesion that almost all the time arises in bone and is also, though rarely, noticed as a secondary phenomenon in certain delicate tissue lesions. Hence, some have proposed the term solid aneurysmal bone cyst for lesions which have large areas of strong tissue with features of giant-cell reparative granuloma and occur in sites typical for aneurysmal bone cyst. Both benign and malignant bone lesions are prone to develop aneurysmal bone cysts as secondary phenomena superimposed on preexisting situations. Large solid arrows point out probably the most frequent areas of the breakpoints within introns. These findings clearly point out that no much less than some aneurysmal bone cysts are true neoplasms with identifiable oncogene and promoter gene mechanisms of growth. In major, or de novo, aneurysmal bone cysts, no underlying condition may be identified radiographically or microscopically. Incidence and Location Aneurysmal bone cyst is relatively rare, accounting for approximately 2. Hence, its virtually uniform skeletal distribution is a novel feature amongst bone tumors. Note that peak incidence of both forms of aneurysmal bone cyst is throughout second decade of life. The major long tubular bones of the higher and decrease extremities account for 20% of the circumstances. The flat bones (the pelvis and scapula) are also well-known places for aneurysmal bone cyst. Lesions that involve the ends and midshaft areas of lengthy bones occur less regularly. Rare examples of multiple metachronous aneurysmal bone cysts in as many as five different skeletal websites have been reported. Occasionally the patient has a relatively brief history of pain and swelling that progressively developed over a few weeks. The vertebral lesions typically current with a full gamut of signs and symptoms associated to compression of the spinal wire and nerves. Radiographic Imaging the radiographic presentation could be very distinctive, and in most cases the prognosis of aneurysmal bone cyst is recommended on the basis of x-ray features. The blowout or expanded element is found overlying an space of cortical disruption. The radiographic features are best understood if the lesion is envisioned as an expansile, multilocular balloon disrupting the adjacent bone and elevating the periosteum. Although uncommon, reactive bone within the lesion may be documented radiographically as lesional calcifications.
AGN (Ascorbigen). Dilantin.
- How does Ascorbigen work?
- Dosing considerations for Ascorbigen.
- What is Ascorbigen?
- Fibromyalgia and breast cancer.
- Are there any interactions with medications?
- Are there safety concerns?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=97112
Buy dilantin visa
Therefore the treating surgeon ought to examine the globe and visible operate to rule out potential ocular or orbital harm. Visual acuity is also measured, and sometimes examination of the fundus is indicated to allow the surgeon to rule out a direct harm to the globe or penetration from a overseas object. Patients could present with a really small eyelid puncture wound or laceration that appears insignificant, but thorough questioning of the patient regarding the mechanisms of harm could reveal the potential for retained overseas bodies that must be investigated. These conditions may not be amenable to acute and even secondary surgical procedure, however it is very important document the extent of harm. Lacerations may extend into the lacrimal canaliculus within the inner corner of the eyelids. Crawford intubation with silicone is a handy method of splinting the canalicular system. C, the swinging flashlight check is used to check for the afferent pupillary defect, which indicates optic nerve damage. In the top determine, the light causes pupil constriction in both eyes, as a result of the alternative pupil has consensual constriction. Consider a retained foreign body (particularly when an natural object strikes the eye); the historical past may be unreliable; assess for occult perforations, a chronic cutaneous fistula, or an unresolved inflammatory process. Chemosis and the hematoma are confined to an space delineated by insertion of the orbital septum (arcus marginalis). Many instances these full-thickness accidents outcome from a wound from a pointy object or as a outcome of a shearing effect, significantly within the inside canthus. To avoid postoperative notching when repairing these defects, the identical principles ought to be followed as for full-thickness eyelid reconstruction of upper and lower lids. If the sides of the wound are irregular and the tarsal plate is fragmented, the tarsal edges may not line up as desired. The lid should then be closed in layers; crucial closure is of the tarsal plate. C, To keep away from lid notching, the tarsal edges should be parallel and prolong the total ver- Preventing adhesions to the orbital rim (lid notChing) Wounds generally extend through the eyelid into deeper tissues within the face or forehead or to the bony orbital rim. After closing a laceration, tarsorrhaphy sutures in line with the laceration may help forestall notching. B, this patient had higher and decrease lid lacerations with adhesions to the inferior rim. B, Appearance after meticulous closure of deep tissue over the orbital rim space to forestall retraction. Attempts to suture and reattach extraneous tags or flaps usually produce only frustration and a less than passable postoperative result. Our suggestion on this situation is to shut deep tissue, trim skin tags and flaps, dermabrade the sides, and allow natural granulation to occur. The lately developed SkinPen is healthier than dermabrasion notably around the eyes with no danger of avulsion, much less ache, and only 24 hours of redness from needling the scar quite than sanding down an entire layer. B and C, Initial end result after closing deep tissue, trimming the skin tags, and permitting pure granulation to fill within the deficits. D, Result after a skin graft to the left upper lid, seen at 6 weeks postoperatively. Chapter 28 � Management of Eyelid and Periorbital Trauma 825 Preserving eyelid tissue Many patients present with intensive accidents and tissue that seems macerated or disconnected from the eyelid or periorbital area. In some circumstances, eyelid tissue is totally indifferent from the patient but fortuitously discovered on the scene of the incident. If debridement of eyelid tissue is important, acute reconstructive procedures may be necessary to preserve globe integrity. C, Same patient 2 months later; the higher lid, regardless of its deficiencies, is protecting the cornea. B, the upper lid was discovered on the scene of the accident; it was positioned in a saline and antibiotic answer and was sent with the patient. E, Injuries in the forehead and glabellar space are debrided and allowed to undergo pure granulation. Absence of the decrease lid also can produce exposure damage to the eye, but many people can tolerate this for longer than a missing upper lid.
Buy genuine dilantin line
C, the cross-sectional anatomy of the inferior oblique muscle, which may be injured throughout a transconjunctival blepharoplasty. E, Retraction of the lateral fringe of the incision, exposing the lateral pocket for removing. Surgeons ought to carefully keep away from the inferior oblique muscle, which is between the medial and nasal fat pad. This is the most incessantly injured muscle throughout transconjunctival decrease blepharoplasty procedures. Cauterization of the edges of the capsulopalpebral fascial layer for hemostasis is often needed. Lateral canthal anchoring is performed in all patients who bear a decrease lid blepharoplasty, as a end result of it provides decrease lid help, facilitates practical eyelid-closure mechanics, and helps to management the shape of the eyelid fissure. The canthus ought to all the time be anchored inside the orbital rim, not at the edge, permitting the lid to conform to the globe. B, Lateral canthal anchoring requires publicity of the lateral orbital rim for fixation of the decrease lid and canthus. The decrease lid is distended from the globe to decide the quantity of lid laxity present. B, the release of the inferior retinaculum facilitates the delicate supraplacement of the canthus. B, If adequate pressure on the lower lid is obtained with this maneuver, a canthopexy is performed. If the lid is distensible and the decrease lid tension is inadequate even after the lateral canthus is tucked against the rim, lid shortening and a canthoplasty are carried out. Some sufferers have residual contour deformity of the canthus after a canthopexy is performed, the end result of both redundancy or distortion. Each arm of the suture is introduced at the desired position inside the orbital rim periosteum. A, A double-armed everlasting suture (4-0 Mersilene with a P-2 needle) is inserted through the lower lid on the lateral canthus and anchored to the orbital rim periosteum. If the lower lid rigidity is enough, the canthopexy is the definitive anchoring process. The advantage of utilizing a dissolvable suture is that the canthopexy suture is probably not needed permanently and prevents the danger of having to remove a suture later because of an infection or irritation. B, A canthoplasty with fixation of the lower lid to the periosteum of the orbital rim mixed with lid shortening. B, A technique of suture insertion in the edge of the lid for fixation to the orbital rim, showing a closeup of the realigned lateral canthal angle. The grey line of the higher and decrease lid and the lash margins should be properly aligned to forestall blunting or webbing of the lateral canthal angle. D, A lateral cantholysis of the lateral retinaculum is performed to free the decrease lid for elevation for canthoplasty. The quantity of decrease lid resection wanted is determined by putting the sting of the lower lid against the lateral periosteum and assessing redundancy. The lid is shortened by full-thickness excision of the redundant lateral lower lid. This suture is then positioned in the internal lateral orbital periosteum on the horizontal pupillary line. The margins of the upper and decrease lids on the canthus are exactly aligned with a 5-0 or 6-0 buried Vicryl suture to guarantee symmetrical lid alignment on the gray line and of the lashes. This technique ensures that the connection of the upper and decrease lid re-creates the "vest-over-pants" anatomy. The lateral scleral triangle is larger and more pointed than the nasal scleral triangle and varies far more with changes in lateral canthal anchoring; these adjustments are simpler within the total context of the decrease lid position and eye prominence. A outstanding or a deep-set eye-particularly when related to a constructive or unfavorable vector, such as a recessed or outstanding malar area-can also affect eye fissure shape, depending on the final place of the canthal anchoring. In sufferers with a recessed malar space, or a unfavorable vector, the tendency is towards a downward clotheslining of the lower lid postoperatively; in sufferers with a prominent malar area, or a constructive vector, the tendency is towards an upward clotheslining of the decrease lid postoperatively. The normal positioning of canthal anchoring is at the middle of the pupil and the position is contained in the orbital rim. B, With a deep-set eye, the decrease lid will clothesline upward, an effect that occurs with superior placement of canthal anchoring at the superior pupil. Altering the point of canthal anchoring to a more downward and inward fixation level contained in the orbital rim at the level of the inferior pupil will prevent this drawback.
Buy discount dilantin 100mg line
However, longitudinal, nonlinear photographic studies by Lambros have proven that though the brow could gain wrinkles and drop, the aged eyebrow often strikes superiorly on the lateral forehead as a end result of the mix of deflation of soft tissue and the motion of the forehead elevator, the frontalis muscle. In many patients, however, notably males with poor forehead support, the brow can even descend, which is clear by a lower in the resting brow-lash distance. B, A temporal carry is carried out via a restricted incision with release of the temporal line of fusion and the orbital retaining ligaments. B, this feminine affected person has good lateral brow place despite activity of the frontalis muscle evident by the transverse forehead rhytids and growing older within the midface. Skin folding in the higher lid is caused by both the lack of elasticity within the skin itself and laxity and descent of the eyebrow. As many people age, the upper eyelid sulcus deepens, and they develop deep-set eyes. Upper lid curvature depends on indentation from the spherical eyeball; as this indentation decreases, the curvature of the higher lid turns into less pronounced. The skin attachments of the aponeurosis commonly stay intact, allowing retraction of the higher lid crease. Age can be a contributing issue to another involutional change that may happen in the levator aponeurosis-dehiscence of the medial horn, which causes lateral migration of the tarsal plate. Because the tarsal plate is not centered on the pupil, this situation may cause flatness of the higher lid. Standard brow laxity and descent ought to be addressed, but different attainable causes have to be recognized. This fullness may be objectionable to patients, and repositioning the gland is sometimes essential. B, Repair by repositioning of the orbital lobe back beneath the superior orbital rim by suturing the lateral horn of the levator on downward stretch to keep away from lagophthalmos to the lateral orbital rim periosteum with a 6-0 Vicryl suture. Patients sometimes complain of lateral fullness; sculpting and thinning the brow fats pad could also be indicated for these individuals. If this prominence is objectionable to the patient, sculpting or thinning the superior lateral rim surgically with a burr ought to be mentioned as an choice. B, A patient with dermatochalasis in the higher lids and early recession of the upper sulcus on the left lid caused by levator dehiscence. C, this patient reveals getting older modifications in the upper lids, with a deep higher sulcus formation attributable to levator dehiscence. Likewise, heredity and/ or repeated swelling and irritation can worsen this process. Fat ProtruSion the loss of integrity in the orbital septum and connective tissues commonly causes the fat compartments within the lower eyelids to protrude. B, Another patient with growing older adjustments; she has extra dermatochalasis than fats herniation. Because of her deep-set eyes and enophthalmos from getting older, the lower lid edge is larger than the limbus. C, the decrease lids of this affected person have lid malposition and tarsoligamentous laxity along the decrease lid margin due to eye prominence, leading to scleral show, tear trough deformity, and malar baggage. With age, this loss of elasticity also affects the tone of the lower lid in opposition to the globe, which in flip causes a lower in vertical and horizontal eyelid actions that are correlated with laxity. The integrity of the lateral canthal tendon profoundly impacts lower lid place, eyelid closure mechanics, and eye fissure shape. Orbicularis oculi hypertrophy may outcome within the improvement of smile traces, presumably due to repeated animation. In the lower lid, however, this curvature is affected by both globe indentation and lateral canthal ligament integrity. As a affected person with deep-set eyes ages, the decrease lid could transfer upward as the lateral scleral triangle narrows, producing a a lot smaller, horizontal eye fissure. In contrast, the lower lid of a patient with extra prominent eyes may generally tend for downward migration, round eye fissure form, and scleral present with age. B, Aging adjustments in a deep-set eye, with an upward movement of the lid and a narrowing of the lateral scleral triangle. C, Aging adjustments in a prominent eye, with a bowing down of the lower lid, which causes scleral show.
Dilantin 100 mg otc
A neurosurgical session is required in emergency situations during which intracranial complications end result from orbital roof fractures. Beyond the primary harm, the development of meningitis or a mind abscess is the major danger in plenty of of these instances. A discussion of the neurosurgical management of those complicated circumstances is past the scope of this textual content. Chapter 35 � Acute Orbital Trauma: Evaluation of Neuroophthalmologic Injuries 1043 Orbital roof fractures can contain the frontal sinus or the nasofrontal duct. Sinus obliteration may be thought of on the time of initial surgical restore to forestall the delayed-onset complication of frontal sinus mucoceles. Rarely, repair of enormous orbital roof defects is critical in patients with vital exophthalmos secondary to orbital herniation of the anterior cerebrum. These giant orbital roof defects are frequently contiguous with a frontal sinus fracture. With an exposed sinus the risk of infection is elevated; due to this fact skinny autologous bone grafts must be used to restore the defect somewhat than alloplastic materials. It may be necessary to scale back displaced bone fragments that mechanically limit the superior rectus muscle or impinge on the levator palpebrae muscle. With blunt trauma, there are different, extra frequent causes of extraocular muscle imbalance and ptosis. In the absence of considerably displaced bony fragments, extraocular muscle surgical procedure and ptosis repair are usually delayed for six months after trauma. This area is quite prone to intracranial injury and injury with superior nasal penetrating trauma. Lacrimal sac mucoceles, dacryocystitis, and epiphora may end up from nasolacrimal obstruction and should require dacryocystorhinostomy to reestablish tear drainage into the nostril. Medial orbital trauma may disrupt attachments of the medial canthal tendon and trigger displacement of the medial canthus and eyelids, leading to traumatic telecanthus. Orbital emphysema and epistaxis are frequent sequelae of medial orbital fractures because of injury to the ethmoid sinus. The frontal sinus usually drains into the nasal cavities via the nasofrontal duct. When seen in surgery, he had a complete rupture of globe and drainage of clear fluid into the socket, as seen on this image. Neurosurgery initially was performed to shut the cranial orbital from the transcranial method with acrylic. Identifying the quadrant of the damage may help to pinpoint the situation of an intraorbital harm such as superior orbital fissure syndrome or orbital apex syndrome. Neurologic trauma causing optic neuropathy is followed by a restricted, 90-minute period to restore normal blood circulate to the retina. A number of neuroophthalmologic injuries can occur and should be dominated in or dominated out in the course of the initial bodily examination. A international physique within the orbit and even intracranially should always be suspected. Overall, complicated, traumatic neuroophthalmologic accidents require quick consultation from a neuroophthalmologist. Indirect traumatic optic neuropathy-visual consequence of operative and nonoperative instances. Ophthalmic elements of orbital harm: a complete diagnostic and management method. A retrospective research of therapy of orbital flooring fractures with the maxillary sinus strategy. Early definitive bone and soft-tissue reconstruction of major gunshot wounds of the face. The pattern and incidence of nasolacrimal injury in naso-orbitalethmoid fractures: the role of delayed assessment and dacryocystorhinostomy. Complications related to alloplastic implants used in orbital fracture restore.
Dilantin 100mg visa
The use of collagen-based fillers has decreased significantly, from a 90% market share in 2000 to solely 2. This chapter critiques probably the most generally used injectable merchandise for facial rejuvenation, indications and contraindications, therapy areas and totally different methods, and issues. Furthermore, the density, G prime lifting force, hydrophilic degree of the filler, colour, and danger of Tyndall discoloration ought to be thought of earlier than making a choice of the location to inject, depth to inject, amount to inject, and which filler has demonstrated the most effective outcome in outlined areas of the periorbital region. The 5 layers for injection include the superficial dermis, middermis, deep dermis, and subcutaneous and preperiosteal layers. Note that a second layer of the eyelid has no subcutaneous layer between the dermis and the orbicularis muscle. Its first medical use was within the late Nineteen Fifties as an alternative selection to eye vitreous fluid, but its first use as a beauty agent was in 1996 in Europe to efface fantastic facial traces. Commercially available hyaluronic acids are produced by extraction from rooster combs (Hylaform) or by synthesis and fermentation of recombinant Streptococcus species or the Bacillus subtilis bacterium. More-viscous preparations (Perlane, Juv�derm Ultra Plus, Voluma) are higher suited for lifting or volume restoration, corresponding to filling cheeks and smile strains. These had been the only obtainable collagen fillers within the Nineteen Eighties and early Nineties earlier than hyaluronic acid fillers turned out there. With 100,000 particles/ml, Restylane is considered a middle ground for particle size/viscosity and is intended for the correction of wrinkles. In comparability, Perlane has 10,000 particles/ml and is meant for filling out deeper folds and for volumizing. A newer filler, Restylane Silk, is indicated for submucosal implantation for lip augmentation and dermal implantation for correction of perioral rhytids. Indications embrace injection into the mid to deep dermis for the correction of average to severe facial wrinkles and folds, similar to nasolabial folds. When compared with different merchandise which would possibly be injected at the similar stage, Belotero produces much less superficial lumpiness and swelling and is thus well suited for such areas because the tear trough or nice vertical lines around the periorbital space. It is a extremely viscous and elastic materials that spreads minimally from its subcutaneous injection website. It has an extended track record of safety in vivo because the precept element of Vicryl suture, resorbable plates and screws, and as a drug delivery car. Although the therapy regimen for lipodystrophy usually consists of three or 4 injection classes spaced 3 weeks apart, many practitioners use only one session when treating wrinkles. The product requires 2 hours to dissolve and may be stored at room temperature (up to 30� C [86� F]) for seventy two hours after reconstitution. The manufacturer recommends injecting the suspension with 26-gauge or bigger needles. Relative contraindications embody sufferers with delicate connective tissue illness and up to date use of fish oil, vitamins, or herbal preparations. Although injection in or around sensory nerves can be painful, thrombotic or embolic problems from inadvertent injection of filler right into a vessel lumen can be catastrophic. C, the periorbital nerves with the primary areas to keep away from during injection include the infraorbital, supraorbital, and supratrochlear nerves. A exact and delicate injection method should be used when treating this space, because inadvertent injection into the supratrochlear artery could cause blindness with retrograde flow of filler to the takeoff of the ophthalmic artery, or glabellar skin necrosis with antegrade circulate of filler. Overcorrection on this area in addition to high fill volumes can compress small vessels supplying blood to the glabellar skin. Chapter 19 � Injectable Fillers 517 When a volume-deficient cheek or nasojugal groove is being treated, the origin of the infraorbital foramen should be marked 10 mm inferior to the palpable zygomaxillary suture, or from a vertical line drawn at the lateral corneoscleral limbus. Aside from thrombotic issues, inadvertent injection of even a small quantity of filler superior to this area deep to the orbital septum could cause persistent edema within the lower eyelids. The zygomaticofacial foramen on the malar eminence should be averted, because injection into the nerve can be fairly painful. The surgeon outlines the therapy options for correction of the problem, together with surgical alternate options. On physical examination, any asymmetries are famous and discussed with the affected person.