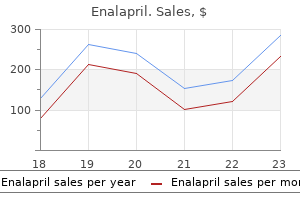
Enalapril dosages: 10 mg, 5 mg
Enalapril packs: 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

Order 5 mg enalapril with mastercard
However, one latest research has shown that same-day discharge remains to be protected in the absence of other comorbidities. The threat for death or readmission within 7 days of surgery in patients over sixty five years of age are 41 per one hundred,000 and a pair of. Overall, older sufferers had a twofold enhance in the threat for intraoperative opposed cardiovascular occasions; however, this was seen not as a contraindication to ambulatory surgical procedure but quite as indicating the necessity for more careful intraoperative management. One research suggests a reduced incidence of postoperative cognitive dysfunction in older patients after ambulatory surgical procedure in comparison with comparable procedures carried out on an inpatient basis,fifty three presumably due to using short-acting anesthetic strategies and reduced separation from their acquainted house setting. At the other age extreme, the decrease restrict for ambulatory surgical procedure may differ depending on the experience and specialization of the person establishment. Although hypertension is a vital risk issue for long-term health, a meta-analysis of nearly thirteen,000 sufferers showed that it elevated the chance for perioperative issues by only one. Angiotensin-converting enzyme inhibitors and angiotensin receptor antagonists are generally withheld on the morning of surgical procedure to forestall hypotension after induction of anesthesia. For minimally invasive procedures, the international normalized ratio may be briefly decreased to the low or subtherapeutic vary, with the standard dose of oral anticoagulation resumed immediately after the procedure. Patients often reside within an affordable touring distance of the surgical unit, however this could be impractical in rural or sparsely populated areas. Patients who select to travel long distances after ambulatory surgery often are very glad with their care. A common security feature is to require all sufferers having surgery under basic anesthesia or sedation to be discharged with a accountable grownup escort and to have somebody stay with them for the next 24 hours. If the 24-hour companion is remitted, sufferers often disregard postoperative directions and send their escorts away if they feel nicely at home. Other than identifying this small group of sufferers, preoperative assessment is primarily required to evaluate and optimize patients and to present applicable data (Table 89-2). These assessment and optimization functions could be further distilled into two key questions: "Is there any benefit to this patient of being in hospital overnight after surgical procedure This becomes increasingly difficult because the interval between the choice to function and the date of surgical procedure turns into shorter. Ideally, preoperative assessment should instantly comply with the choice to operate, by providing a "one-stop shop. An alternative is to use a fundamental screening software to establish these patients who can proceed directly to surgery and those who require additional investigation or administration. Identify absolute contraindications to ambulatory surgical procedure Examples Inability to establish a accountable caregiver other than for minor surgery with full and speedy recovery anticipated; extreme uncorrectable cardiovascular disease Patient requires additional investigation, therapeutic modification, or intervention to improve functional status; identify a pal, relative or neighbor to act as caregiver Potentially difficult intubation necessitating advanced airway management abilities; malignant hyperpyrexia�susceptible affected person requiring trigger-free anesthetic; latex allergy; obese affected person requiring operating table/trolley with high weight restrict and additional width Written info on preoperative preparation, treatment administration, preoperative fasting, etc. Screening permits many sufferers to undergo assessment by telephone or questionnaire, with clinic attendance required provided that surprising problems are uncovered or if requested by the patient. When telephone assessment was chosen for all young wholesome patients scheduled for minor breast surgery, only 2% of patients had issues recognized that required further evaluation within the ambulatory surgery middle. In distinction, advance face-to-face preoperative assessment is more advisable for older patients, in whom a number of comorbidities, polypharmacy, and social issues are all more probably. More complex sufferers have their anesthesia preassessment performed by an anesthesiologist. A comprehensive preoperative history and bodily analysis by a nurse practitioner is commonly additionally provided in the preoperative evaluation clinic for the surgeon. Using a nurse practitioner to help in preoperative analysis maintains patient safety and satisfaction, frees priceless sources, and will increase employees satisfaction. Yes Telephone or questionnaire evaluation No Preoperative Assessment Clinic No Can care be organized with a pal or relative Yes Condition(s) only probably No to trigger problems during and/or soon after surgical procedure Flowchart illustrating the fundamental process for selecting patients for ambulatory surgical procedure. The pathway incorporates a screening process for patients who may not require a full faceto-face assessment in the clinic. In Radford M, Williamson A, Evans C, editors: Preoperative evaluation and perioperative administration, Cumbria, Calif, 2011, M&K Books, with permission. No Schedule for ambulatory surgical procedure Yes Ensure suitable anesthesiologist and/or facilities can be found Schedule for inpatient surgical procedure Chapter 89: Ambulatory (Outpatient) Anesthesia 2619 useful information could be obtained from the historical past, supplemented by easy statement of the patient. Ten sufferers with severe aortic stenosis (valve space 1 cm2 or much less, gradient 35 to 58 mm Hg) tolerated an unmodified anesthesia routine for electroconvulsive remedy on one hundred forty four occasions with out issues,88 suggesting that ambulatory surgical patients with undiagnosed aortic stenosis might not inevitably be at excessive risk, when mixed with acceptable procedure choice. Many patients are disproportionately nervous about extremely unlikely outcomes, similar to dying and awareness,95 yet considerably less concerned about extra frequent consequences corresponding to nausea, vomiting, and postoperative discomfort.
10 mg enalapril sale
The subcutaneous block was carried out by a single injection with a 25-gauge needle into the palmar skin on the base of the finger. The lumbar plexus lies within the psoas compartment in the paravertebral house, with the anterior border shaped by the psoas major muscle and the posterior border shaped by the quadratus lumborum muscle. Landmarks of psoas compartment block with totally different procedures described within the pediatric literature. These nerves run a variable a half of their course slightly below the fascia iliaca, which is the common fascia overlaying psoas and iliacus muscle. A sufficient volume of native anesthetic injected on the inner surface of this fascia will unfold along it and attain these nerves, thus producing a fascia iliaca compartment block. Psoas Compartment Block (Direct Lumbar Plexus Block) Psoas compartment block is carried out with the kid turned within the lateral decubitus place with the operated aspect uppermost. The landmarks are the iliac crests, the ipsilateral posterior superior iliac backbone, and the L5 spinous course of. The midpoint of the line becoming a member of the posterior iliac spine to the L5 spinous course of (modified Chayen approach) 2. A level located on the intercristal line (Tuffier line), three quarters of the gap between the spinous strategy of L4 and a line parallel to the spinal column passing by way of the posterior superior iliac spine235 three. A level positioned at medial two thirds and the lateral one third on a line from spinous means of L4 to the posterior superior iliac spine236 Whatever the puncture web site used, the block needle is inserted perpendicularly to the pores and skin till twitches are elicited in the ipsilateral quadriceps muscle. Complications, together with cardiac arrest from intravascular injection, psoas muscle hematomas, epidural anesthesia, and retroperitoneal injection if the needle is inserted deeper than beneficial, have been reported. The ordinary indications for this block are surgical procedures on the hip or femoral shaft (femoral and hip osteotomies). These operations require blockade of the three main nerves innervating the hip joint: femoral, lateral femoral cutaneous, and obturator nerves. Psoas compartment block can produce wonderful postoperative pain administration through the first 48 hours. A recent research using sonography of the lumbar plexus in kids showed that the depth of the lumbosacral plexus correlated with weight quite than age. Femoral Nerve Block Femoral nerve blocks are carried out whereas the child lies supine, preferably with the ipsilateral limb barely abducted. The block needle is inserted posteriorly, both perpendicular to the anterior side of the thigh or, especially when a catheter has to be inserted, at a 45-degree angle cephalad, pointing to the umbilicus, until twitches are elicited within the quadriceps muscle when neurostimulation is used. The introduction of a catheter for continuous analgesia could be achieved by the direct perivascular (femoral) approach241 or the fascia iliaca compartment strategy. Fascia Iliaca Compartment Blocks the approach consists of injecting an area anesthetic below the fascia iliaca. With this method, the femoral and lateral cutaneous nerves are nearly continuously blocked. The native anesthetic usually reaches the upper division department of the obturator nerve, which is the branch giving a twig to the hip joint. The anesthetized area also includes areas provided by higher branches of the lumbar plexus in more than 70% of procedures, such because the genitofemoral nerve. Perivascular femoral nerve and fascia iliaca compartment approaches have by no means been compared when it comes to efficacy in children. Performing this block utilizing ultrasound showed several benefits, including extension of the duration of postoperative analgesia and reduce within the volume of injected local anesthetic in distinction to that with neurostimulation method. The length of analgesia was considerably elevated to roughly Chapter ninety two: Regional Anesthesia in Children 2739 508/178 minutes versus approximately 335/69 minutes for all blocks using the same strategies. Local anesthetics with epinephrine Needle Fascia iliaca Fascia lata produce considerably decrease plasma concentrations and must be most popular each time attainable. Addition of clonidine (1 to 2 g/kg) significantly prolongs the length of analgesia. Recently, Lako and associates243 in contrast continuous fascia iliaca block and intravenous morphine in phrases of analgesia and unwanted effects in children present process pelvic osteotomy. The authors noted wonderful postoperative pain reduction, with much less sedation and a better return of appetite within the regional analgesia group in contrast to the morphine group. On the opposite hand, Paut and colleagues242 decided plasma concentrations of bupivacaine throughout steady fascia iliaca block in youngsters after main femur or knee surgical procedure or femoral fracture. They concluded that the plasma concentrations of bupivacaine throughout continuous fascia iliaca compartment block are within the security margins for children (0. Saphenous nerve blocks are used as a complement to sciatic blocks with small amounts of local anesthetic.
10mg enalapril with amex
Dizdarevic K, Hamdan A, Omerhodzic I, Kominlija-Smajic E: Modified Lund concept versus cerebral perfusion pressure-targeted remedy: a randomised managed research in patients with secondary mind ischaemia, Clin Neurol Neurosurg 114:142-148, 2012. Sadaka F, Veremakis C: Therapeutic hypothermia for the management of intracranial hypertension in extreme traumatic mind damage: a scientific review, Brain Inj 26:899-908, 2012. Denson K, Morgan D, Cunningham R, et al: Incidence of venous thromboembolism in sufferers with traumatic brain injury, Am J Surg 193:380-383, 2007. Ransom E, Mocco J, Komotar R, et al: External ventricular drainage response in poor grade aneurysmal subarachnoid hemorrhage: impact on preoperative grading and prognosis, Neurocritical Care 6:174-180, 2007. Roos Y, Rinkel G, Vermeulen M, et al: Antifibrinolytic therapy for aneurysmal subarachnoid hemorrhage: a significant replace of a Cochrane evaluate, Stroke 34:2308-2309, 2003. Suhardja A: Mechanisms of disease: roles of nitric oxide and endothelin-1 in delayed cerebral vasospasm produced by aneurysmal subarachnoid hemorrhage, Nat Clin Pract Cardiovasc Med 1: 110-116, 2004. Gruber A, Reinprecht A, Gorzer H, et al: Pulmonary function and radiographic abnormalities related to neurological outcome after aneurysmal subarachnoid hemorrhage, J Neurosurg 88:28-37, 1998. Charpentier C, Audibert G, Guillemin F, et al: Multivariate analysis of predictors of cerebral vasospasm prevalence after aneurysmal subarachnoid hemorrhage, Stroke 30:1402-1408, 1999. Berendes E, Walter M, Cullen P, et al: Secretion of mind natriuretic peptide in patients with aneurysmal subarachnoid haemorrhage, Lancet 349:245-249, 1997. Igarashi T, Moro N, Katayama Y, et al: Prediction of symptomatic cerebral vasospasm in patients with aneurysmal subarachnoid hemorrhage: relationship to cerebral salt losing syndrome, Neurol Res 29:835-841, 2007. Kasuya H, Onda H, Yoneyama T, et al: Bedside monitoring of circulating blood volume after subarachnoid hemorrhage, Stroke 34:956-960, 2003. Kasuya H, Kawashima A, Namiki K, et al: Metabolic profiles of sufferers with subarachnoid hemorrhage treated by early surgical procedure, Neurosurgery 42:1268-1274, 1998. Kansara A, Pandey P, Tiwari A, et al: Stenting of acute and subacute intracranial vertebrobasilar arterial occlusive lesions, J Neurointerv Surg 4:274-280, 2012. Egge A, Waterloo K, Sjoholm H, et al: Prophylactic hyperdynamic postoperative fluid remedy after aneurysmal subarachnoid hemorrhage: a medical, potential, randomized, controlled examine, Neurosurgery 49:593-605, 2001. Muench E, Horn P, Bauhuf C, et al: Effects of hypervolemia and hypertension on regional cerebral blood circulate, intracranial strain, and brain tissue oxygenation after subarachnoid hemorrhage, Crit Care Med 35:1844-1851, 2007. Levine J, Kofke A, Cen L, et al: Red blood cell transfusion is associated with an infection and extracerebral complications after subarachnoid haemorrhage, Neurosurgery sixty six:312-318, 2010. Sanchez-Pe�a P, Nouet A, Claren�on F, et al: Atorvastatin decreases computed tomography and S100-assessed brain ischemia after subarachnoid aneurysmal hemorrhage: a comparative research, Crit Care Med forty:594-602, 2012. Wagner S, Schnippering H, Aschoff A, et al: Suboptimum hemicraniectomy as a cause of extra cerebral lesions in patients with malignant infarction of the middle cerebral artery, J Neurosurg ninety four:693-696, 2001. Rhondali O, Genty C, Halle C, et al: Do sufferers still require admission to an intensive care unit after elective craniotomy for mind surgical procedure Broderick J, Connolly S, Feldmann E, et al: Guidelines for the administration of spontaneous intracerebral hemorrhage in adults: 2007 update: a tenet from the American Heart Association/American Stroke Association Stroke Council, High Blood Pressure Research Council, and the Quality of Care and Outcomes in Research Interdisciplinary Working Group, Stroke 38:2001-2023, 2007. Hypothermia After Cardiac Arrest Study Group: Mild therapeutic hypothermia to improve the neurologic outcome after cardiac arrest, N Engl J Med 346:549-556, 2002. Madl C, Kramer L, Domanovits H, et al: Improved end result prediction in unconscious cardiac arrest survivors with sensory evoked potentials compared with scientific assessment, Crit Care Med 28:721-726, 2000. Cosi V, Versino M: Guillain-Barr� syndrome, Neurol Sci 27(Suppl 1): S47-S51, 2006. Humans are adaptable organisms with many interrelated mechanisms that identify, reply, and neutralize each inner. Anesthesiologists should be educated about these mechanisms because they routinely care for patients with acute and continual homeostatic modifications. The stress response developed as a way for serving to organisms react to quick danger. Metabolic alterations attributable to adjustments within the hormonal milieu increase the availability of certain substrates and reduce the availability of others. For example, amongst sufferers with underlying coronary artery illness, the tachycardia and increased myocardial oxygen demand ensuing from catecholamine stimulation may cause myocardial ischemia. The stress response was initially described by Hans Selye as "the nonspecific response of the physique to any demand upon it. Furthermore, chronic activation of the stress response has been implicated as contributing to a wide selection of situations, similar to atherosclerosis and depression.
Generic 5 mg enalapril mastercard
Standard intensive care displays can be utilized to provide simultaneous measurement of arterial and pulmonary artery pressures and intermittent measurement of cardiac output by thermodilution. If stress bags are used to drive continuous circulate methods, they should be repressurized throughout compression and vented earlier than or during decompression. Pulmonary artery catheter balloon ports also wants to be left open to the chamber throughout compression and decompression. Defibrillation could generate a fireplace if sparking occurs or combustible materials are current within the vicinity of the paddles (see also Chapter 109). Despite the fear of inflicting hearth, defibrillation has been carried out in multiplace chambers quite a few occasions with out arcing, fire, or explosion. Most intravenous infusion pumps work properly inside a hyperbaric chamber at pressure (although electrical issues of safety exist; see later). Glass bottles are greatest excluded from the chamber because of the chance of explosive rupture during decompression. Check valves can forestall unintended backflow of blood from the patient within the occasion of disconnection of the pump. Rigid arterial stress transducer tubing helps to forestall kinking whereas the affected person is contained in the chamber. Measured versus predicted partial arterial strain of oxygen (PaO2) at increased ambient stress. It is clear that PaO2 predicted in this method is close to the actual measured PaO2. Proceedings of the ninth international symposium on underwater and hyperbaric physiology, Bethesda, Md, 1987, Undersea and Hyperbaric Medical Society, p 1127. Blood gas rigidity measurement should therefore ideally be carried out inside the hyperbaric chamber through the use of an appropriately calibrated analyzer. The ideal necessities for ventilation embrace small dimension, no electrical requirement, absence of flammable lubricants, ability to operate on a volume-cycled foundation over a variety of tidal volumes and respiratory charges, minimal modification requirement for installation, and ability to present optimistic end-expiratory pressure, as properly as to ventilate in intermittent obligatory air flow and assist/control modes. As ambient pressure increases, fuel density is proportionately increased, whereas relatively little change happens in gas viscosity. Measurements of respiratory conductance (the reciprocal of resistance) throughout tidal breathing160 point out that it varies with gasoline density according to the following method: G = G0 k the place G is lung conductance at gasoline density, G0 is the conductance at gasoline density 1. In addition, the upper fuel density ends in a much less environment friendly distribution of ventilation, manifested by an increase in physiologic lifeless space. Several forms of ventilators have been used and tested in hyperbaric chambers (see additionally Chapter 103). Pressurecycled gadgets have been used with some success as a end result of their compactness admirably fulfills the requirement for small dimension. However, continuous adjustment of fee and cycling strain is critical with modifications in ambient strain. Volume-cycled ventilators seem to work well,159,162 although at increased stress some adjustments in fee might occur. First, in any ventilator delivering enriched O2, a possible fire hazard may result from O2 buildup throughout the ventilator case or leakage of O2 into the chamber. Air-filled endotracheal tube cuffs tend to lose quantity during compression and reexpand throughout decompression. Appropriate cuff inflation quantity could be maintained both by manually adjusting the air stress inside the cuff during compression and decompression or by filling the cuff with water. In others, the concentration is assumed to be high due to a excessive rate of O2 circulate by way of the top tent. Leakage of O2 from head tents, masks, and ventilators tends to elevate the chamber O2 focus. Typically an higher restrict of approximately 23% is used as a criterion for ventilating the chamber with air or small volumes of 100% nitrogen until the O2 concentration decreases. Volatile gases such as alcohol vapor from skin disinfectant solutions and mercury vapor from spillage of sphygmomanometer columns may also pollute the atmosphere.
Buy enalapril line
A potential study involving 128 youngsters older than 5 years of age reported a ninety. Another prospective research involving 58 kids (age vary, 7 to 12 years) present process lower extremity orthopedic surgical procedure compared steady epidural infusion of 0. Because sacral interspaces stay nonfused until early adulthood, the sacral epidural space of youngsters may be approached posteriorly via the S2-S3 interspace, which is recognized by palpation zero. Because sacral spinous processes are atrophic, the Tuohy needle may be oriented cephalad or, ideally, caudad to contact the dura mater with the convex a half of the needle tip, thus lowering the hazard of unintentional dural penetration. Attention should be paid to the nearer skin proximity of the epidural space, in contrast to lumbar approaches. If necessary, an epidural catheter may be inserted (using the same approach as for lumbar epidural catheter placement) to present long-lasting postoperative pain relief. Sacral epidural anesthesia is a substitute for caudal anesthesia, both in infants when pores and skin lesions contraindicate a caudal method or in children older than 6 to 7 years of age, in whom caudal anesthesia turns into tougher and fewer dependable. The identical volumes and doses of native anesthetic as for a caudal anesthesia are administered. Ultrasound imaging can be used to exactly evaluate the distance from pores and skin to epidural house and, in infants mainly, visualize both the development of the needle and catheter and the unfold of the native anesthetic. Thoracic epidural blocks are indicated for main operations requiring long-lasting ache reduction, thus requiring placement of an epidural catheter to allow repeat injections or continuous infusion of native anesthetic. In youngsters younger than 1 12 months of age, the process is much like that for a lumbar strategy, with needle insertion perpendicular to the spinous process line, because the spine shows a single flexure, especially when bent. As the patient grows and the flexure develops, the method turns into progressively much like thoracic approaches in adults, requiring cephalic orientation of the Tuohy needle up to a 45-degree angle to the skin. In infants, ultrasonography makes seen the dura mater, the progression of the Tuohy needle, and, in many instances, the progression and last place of the tip of the epidural catheter. Very hardly ever, the approach may be contemplated for sufferers with chronic ache or to stop phantom limb pain earlier than an amputation of the upper arm at the scapular level (osteosarcoma of humerus), which is completed virtually exclusively in adolescents. This has appreciable pharmacokinetic consequences and explains why larger doses of local anesthetics are required for spinal anesthesia in infants and younger kids. Children older than 5 years of age behave like adults after spinal anesthesia, whereas younger patients remain hemodynamically secure, with out vital hypotension or bradycardia,200 even in cases of cardiac malformations. Similar results with concomitant decrease in cerebral blood move have been reported in former preterm infants of 41 weeks of postconceptual age. Other indications are scarce, primarily for elective decrease stomach or lower extremity surgery207-209 and, sometimes, for cardiac surgery or cardiac catheterization,210,211 however these indications are controversial. It can be carried out with the affected person within the lateral decubitus position or sitting. Currently, hyperbaric tetracaine and bupivacaine are probably the most generally used local anesthetics. The older the child, the decrease is the dose required; in children between 6 months and 14 years, zero. Clonidine 1 g/kg, fentanyl 1 g/kg, and morphine 4 to 5 g/kg are reported in the pediatric literature as adjuvants to improve the spinal block length (see Table 92-9). Adverse Effects and Complications Spinal anesthesia is technically tough in neonates and infants; the general failure rate ranges from 10% to 25%. Postdural puncture headache is rare in youngsters youthful than 8 years of age but not exceptional, and its incidence may be increased with use of pencil-point spinal needles. Roots emerge from the intervertebral foramina throughout the interscalene area (between the scalene anterior and scalene middle muscle). As in adults, brachial plexus nerve fibers redistribute first to three trunks (superior, center, and inferior), then to three divisions between the clavicle and the primary rib. These divisions recombine and surround the axillary artery as three cords and are named according to their relation to the artery as the lateral, medial, and posterior cords. Because of this sophisticated redistribution of nerve fibers, distribution of anesthesia varies significantly depending on the level at which the native anesthetic is injected. Chapter ninety two: Regional Anesthesia in Children 2729 is important to predict the extension of the motor and sensory block and to determine the most acceptable strategy for a given surgical procedure. The most necessary anatomic distinction between infants and adults pertains to the higher part of the lung and apical pleura that penetrates the neck, above the plane fashioned by the clavicle and first rib (superior thoracic aperture).
Althaeae radi (Marshmallow). Enalapril.
- Sores, skin inflammation, burns, wounds, insect bites, chapped skin, diarrhea, constipation, stomach and intestinal ulcers, irritation of the mouth and throat, dry cough, and other conditions.
- What is Marshmallow?
- How does Marshmallow work?
- Are there any interactions with medications?
- Dosing considerations for Marshmallow.
- Are there safety concerns?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96755
Purchase enalapril canada
This is particularly true for the usage of a serotonin antagonist, which may in any other case be an effective rescue option without sedative unwanted effects. From proceedings of the 2010 annual meeting of the American Society of Anesthesiologists. Palazzo M, Evans R: Logistic regression analysis of fastened patient elements for postoperative sickness: a model for risk assessment, Br J Anaesth 70:135-140, 1993. Koivuranta M, Laara E, Snare L, Alahuhta S: A survey of postoperative nausea and vomiting, Anaesthesia fifty two:443-449, 1997. Stadler M, Bardiau F, Seidel L, et al: Difference in threat components for postoperative nausea and vomiting, Anesthesiology 98:46-52, 2003. Sherman C: Motion illness: review of causes and preventive strategies, J Travel Med 9:251-256, 2002. Hovorka J, Korttila K, Erkola O: the expertise of the person ventilating the lungs does affect postoperative nausea and vomiting, Acta Anaesthesiol Scand 34:203-205, 1990. Kerger H, Mascha E, Radke O, et al: Does nasogastric tube use reduce the chance of postoperative nausea and vomiting Breitfeld C, Peters J, Vockel T, et al: Emetic results of morphine and piritramide, Br J Anaesth ninety one:218-223, 2003. Gupta A, Stierer T, Zuckerman R, et al: Comparison of restoration profile after ambulatory anesthesia with propofol, isoflurane, sevoflurane and desflurane: a systematic review, Anesth Analg 98:632-641, 2004. Macario A, Dexter F, Lubarsky D: Meta-analysis of trials comparing postoperative restoration after anesthesia with sevoflurane or desflurane, Am J Health Syst Pharm 62:63-68, 2005. Kredel M, Goepfert C, Bassi D, et al: the influence of the weather and the phase of the moon on post-operative nausea and vomiting, Acta Anaesthesiol Scand 50:488-494, 2006. Klosterhalfen S, Kellermann S, Pan F, et al: Effects of ethnicity and gender on movement illness susceptibility, Aviat Space Environ Med 76:1051-1057, 2005. Erhardt S, Schwieler L, Engberg G: Excitatory and inhibitory responses of dopamine neurons in the ventral tegmental area to nicotine, Synapse 43:227-237, 2002. Junger A, Hartmann B, Benson M, et al: using an anesthesia data administration system for prediction of antiemetic rescue treatment at the postanesthesia care unit, Anesth Analg ninety two:1203-1209, 2001. Cann C, Curran J, Milner T, Ho B: Unwanted effects of morphine6-glucoronide and morphine, Anaesthesia fifty seven:1200-1203, 2002. Wallenborn J, Rudolph C, Gelbrich G, et al: the impact of isoflurane, desflurane, or sevoflurane on the frequency and severity of postoperative nausea and vomiting after lumbar disc surgical procedure, J Clin Anesth 19:180-185, 2007. Tarkkila P, Isola J: A regression mannequin for identifying sufferers at excessive threat of hypotension, bradycardia and nausea during spinal anesthesia, Acta Anaesthesiol Scand 36:554-558, 1992. Efficacy and harm of antiemetic interventions, and methodological points, Acta Anaesthesiol Scand forty five:4-13, 2001. Recommendations for prevention and treatment, and research agenda, Acta Anaesthesiol Scand 45:14-19, 2001. Murphy E: Metoclopramide also acts at serotonin receptors, Anaesth Intensive Care 35:447, 2007. Melnick B, Sawyer R, Karambelkar D, et al: Delayed side effects of droperidol after ambulatory basic anesthesia, Anesth Analg sixty nine:748-751, 1989. Altorjay A, Melson T, Chinachoit T, et al: Casopitant and ondansetron for postoperative nausea and vomiting prevention in ladies at high danger for emesis: a phase three research, Arch Surg 146:201-206, 2011. Visalyaputra S, Petchpaisit N, Somcharoen K, Choavaratana R: the efficacy of ginger root within the prevention of postoperative nausea and vomiting after outpatient gynaecological laparoscopy, Anaesthesia fifty three:506-510, 1998. Chaiyakunapruk N, Kitikannakorn N, Nathisuwan S, et al: the efficacy of ginger for the prevention of postoperative nausea and vomiting: a meta-analysis, Am J Obstet Gynecol 194:95-99, 2006. Korttila K, Clergue F, Leeser J, et al: Intravenous dolasetron and ondansetron in prevention of postoperative nausea and vomiting: a multicenter, double-blind, placebo-controlled examine, Acta Anaesthesiol Scand 41:914-922, 1997. Mikawa K, Takao Y, Nishina K, et al: Optimal dose of granisetron for prophylaxis towards postoperative emesis after gynecological surgery, Anesth Analg eighty five:652-656, 1997. Brandstrup B: Effects of intravenous fluid restriction on postoperative complications: comparability of two perioperative fluid regimens: a randomized assessor-blinded multicenter trial, Ann Surg 238:641-648, 2003. Nisanevich V, Felsenstein I, Almogy G, et al: Effect of intraoperative fluid management on consequence after intraabdominal surgery, Anesthesiology 103:25-32, 2005. Fassoulaki A, Papilas K, Sarantopoulos C, Zotou M: Transcutaneous electrical nerve stimulation reduces the incidence of vomiting after hysterectomy, Anesth Analg seventy six:1012-1014, 1993. Sossai R, Johr M, Kistler W, et al: Postoperative vomiting in youngsters: a persisting unsolved drawback, Eur J Pediatr Surg three:206-208, 1993. Rusch D, Happe W, Wulf H: Postoperative nausea and vomiting following stabismus surgery in kids: inhalation anesthesia with sevoflurane-nitrous oxide in comparison with intravenous anesthesia with propofol-remifentanil, Anaesthesist 48:80-88, 1999, [in German].
Syndromes
- Dialysis may improve symptoms.
- Pustular -- White blisters are surrounded by red, irritated skin.
- Acetaminophen relieves fever and headaches, and other common aches and pains. It does not relieve inflammation.
- Congestive heart failure is also very common in the elderly. In people older than 75, congestive heart failure occurs 10 times more often than in younger adults.
- Nonsteroidal anti-inflammatory drugs (NSAIDs)
- India
- Abruptio placentae
Cheap enalapril 5 mg with mastercard
Pelosi P, Goldner M, McKibben A, et al: Recruitment and derecruitment throughout acute respiratory failure: an experimental examine, Am J Respir Crit Care Med 164:122-130, 2001. Grasso S, Terragni P, Mascia L, et al: Airway pressure-time curve profile (stress index) detects tidal recruitment/hyperinflation in experimental acute lung injury, Crit Care Med 32:1018-1027, 2004. Grasso S, Mascia L, Del Turco M, et al: Effects of recruiting maneuvers in sufferers with acute respiratory misery syndrome ventilated with protecting ventilatory technique, Anesthesiology ninety six:795-802, 2002. Gattinoni L, Chiumello D, Carlesso E, et al: Bench-to-bedside evaluation: chest wall elastance in acute lung injury/acute respiratory distress syndrome sufferers, Crit Care eight:350-355, 2004. Chiumello D, Carlesso E, Cadringher P, et al: Lung stress and strain throughout mechanical air flow for acute respiratory distress syndrome, Am J Respir Crit Care Med 178:346-355, 2008. Hedenstierna G: Esophageal strain: benefit and limitations, Minerva Anestesiol seventy eight:959-966, 2012. Broseghini C, Brandolese R, Poggi R, et al: Respiratory mechanics during the first day of mechanical air flow in sufferers with pulmonary edema and chronic airway obstruction, Am Rev Respir Dis 138:355-361, 1988. Anonymous: ventilation with decrease tidal volumes as compared with conventional tidal volumes for acute lung harm and the acute respiratory misery syndrome. The Acute Respiratory Distress Syndrome Network, N Engl J Med 342:1301-1308, 2000. Roupie E, Lepage E, Wysocki M, et al: Prevalence, etiologies and end result of the acute respiratory distress syndrome among hypoxemic ventilated patients. Abraham E: Neutrophils and acute lung harm, Crit Care Med 31 (4 Suppl):S195-199, 2003. Holzgraefe B, Broome M, Kalzen H, et al: Extracorporeal membrane oxygenation for pandemic H1N1 2009 respiratory failure, Minerva Anestesiol seventy six:1043-1051, 2010. Roch A, Lepaul-Ercole R, Grisoli D, et al: Extracorporeal membrane oxygenation for severe influenza A (H1N1) acute respiratory misery syndrome: a prospective observational comparative examine, Intensive Care Med 36:1899-1905, 2010. Muller T, Philipp A, Luchner A, et al: A new miniaturized system for extracorporeal membrane oxygenation in grownup respiratory failure, Crit Care 13, 2009. Gattinoni L, Tognoni G, Pesenti A, et al: Effect of susceptible positioning on the survival of patients with acute respiratory failure, N Engl J Med 345:568-573, 2001. Mancebo J, Fernandez R, Blanch L, et al: A multicenter trial of prolonged prone air flow in extreme acute respiratory distress syndrome, Am J Respir Crit Care Med 173:1233-1239, 2006. Rationale, indications, and limits, Am J Respir Crit Care Med 188:1286-1293, 2013. Brochard L, Mancebo J, Wysocki M, et al: Noninvasive air flow for acute exacerbations of persistent obstructive pulmonary illness, N Engl J Med 333:817-822, 1995. Vitacca M, Clini E, Pagani M, et al: Physiologic effects of early administered masks proportional help ventilation in sufferers with persistent obstructive pulmonary illness and acute respiratory failure, Crit Care Med 28:1791-1797, 2000. Lenique F, Habis M, Lofaso F, et al: Ventilatory and hemodynamic results of continuous optimistic airway pressure in left heart failure, Am J Respir Crit Care Med 155:500-505, 1997. Nava S, Carbone G, DiBattista N, et al: Noninvasive ventilation in cardiogenic pulmonary edema: a multicenter randomized trial, Am J Respir Crit Care Med 168:1432-1437, 2003. Lewandowski K: Extracorporeal membrane oxygenation for extreme acute respiratory failure, Crit Care (Lond) four:156-168, 2000. Bautista E, Chotpitayasunondh T, Gao Z, et al: Clinical features of pandemic 2009 influenza A (H1N1) virus infection, N Engl J Med 362:1708-1719, 2010. Chiumello D, Gallazzi E, Marino A, et al: A validation research of a model new nasogastric polyfunctional catheter, Intensive Care Med 37:791-795, 2011. Dembinski R, Hochhausen N, Terbeck S, et al: Pumpless extracorporeal lung help for protective mechanical air flow in experimental lung injury, Crit Care Med 35:2359-2366, 2007. MacNee W: Pathophysiology of cor pulmonale in continual obstructive pulmonary illness. Food and Drug Administration for the remedy of hypoxic respiratory failure associated with scientific or echocardiographic proof of pulmonary hypertension in newborns (also see Chapter 95). The variability of dilator response is likely to be related to the steadiness of pulmonary vascular transforming and active vasoconstriction. Unfortunately, remedy of pulmonary hypertension with intravenous vasodilators might worsen the systemic hypotension. Food and Drug Administration in 1999, by the European Medicine Evaluation Agency and European Commission in 2001, and by the Ministry of Health, Labour and Welfare in Japan in 2008. Enhancement of Ventilation-Perfusion Matching by Nitric Oxide Inhalation the intrapulmonary distribution of blood flow and ven tilation (ventilation-perfusion [V/Q] distribution) is a serious determinant of the efficiency of transpulmonary oxygenation and determines the partial arterial strain of oxygen (PaO2). The shunt from the right to the left side of the circulation is principally extrapulmonary.
Discount enalapril 5mg with mastercard
In general, bias associated with scientific literature�based evidence can arise from five main sources: (1) the article selection protocol, (2) the evaluation process, (3) the reporting of findings from a predetermined type of article, (4) the analysis of research design and statistical techniques, and (5) the grading or weighting of study high quality. Practical countermeasures instituted for every type of bias are described within the following subsections. Selected knowledge from American Society of Anesthesiologists: Practice pointers for central venous catheterization, Anesthesiology 116:539-573, 2012. Detailed information could be discovered within the information extraction workbook of the Guidelines. This range helps be certain that the set of articles selected by the task force is as complete as attainable. Article selection bias can even arise when editorials, letters, and place papers are used as sources of scientific evidence. These types of articles are often written to promote a selected point of view regarding an intervention or outcome of concern. The authors of these articles might or may not be experts, could depend on a narrowly chosen subset of the literature, or could have deliberately written the article to be "controversial. Such a reviewer is most likely not absolutely cognizant of the constraints of the data or the correct context for analyzing and interpreting the reported findings. Ideally, several people, including at least one clinician from each related subspecialty, ought to independently evaluation all of the literature. However, when a number of hundred research should be reviewed, time and cost constraints prohibit such scrutiny. This reliability examine entails the independent review of a randomly chosen sample of articles by at least two methodologists. To verify whether bias has been launched into the review process, a formal reliability evaluation is performed using a predetermined reliability form. The data collected on this kind is then assessed utilizing sensitivity analysis,12-17 and the findings obtained from this reliability assessment are reported in the guideline. Sometimes referred to as reporting the "finest obtainable literature," this form of bias attributes greater significance to certain forms of literature. Random allocation helps make certain that the reported findings are comparatively unaffected by unmeasured risk elements or subject (patient) characteristics. Additionally, it could be very important assess whether or not essential modifications have occurred in the examine population through the course of the study and to be certain that the examine population adequately represents an necessary medical inhabitants. Although many of these potential points reside outdoors the area of the duty force, the last issue related to the clinical salience of research populations is instantly addressed by the duty force when precisely stipulating the major target of the guideline. Nonrandomized prospective studies, even those designed to minimize selection bias. In an try to regulate or management for confounding options of observational research, various statistical strategies, such as linear modeling with covariate changes and propensity rating analysis, can be used. To present a complete blend of proof, the total vary of outcomes have to be reported no matter research design. When a portion of this info is lacking, the assigned grade can be directly affected. For example, a well-designed, double-blind study could omit information pertinent to concealment of allocation. Even if the examine did, in fact, successfully conceal allocation, it will not be mirrored within the assigned grade as a outcome of this data was not reported within the printed article. Realistically, little could be done to manage this sort of bias other than focusing on the aggregated studies as a excessive quality indicator. In addition, attributing a single weight to an intervention risks the introduction of bias as a result of interventions are sometimes associated with any variety of qualitatively totally different outcomes. A reviewer must then decide which of the outcomes is the more clinically necessary. Separate findings for every outcome discovered to be related to an intervention are then reported in the document. Finally, bias in high quality assessment may also be generated when the reviewer is influenced by elements extraneous to the deserves of the examine under evaluate.
Cheap 10 mg enalapril amex
Staffing should be flexible enough to present one-on-one patient care when necessary. A multidisciplinary in-service program is essential for persevering with education and orientation. Other team members include respiratory therapists, physical therapists, nutritionists, social employees, laboratory technologists, pharmacists, and psychiatrists and psychologists for the patients and workers. All medical and support personnel should be encouraged to participate in rounds, instructional endeavors, and group meetings whenever attainable. There must be sufficient workspace round every mattress and sufficient space for storing to maintain life-support equipment within reach. Space for reading, meeting, sleeping, and showering should be out there for the employees members. Space should be offered for fogeys to remain with their kids in the course of the day and for fogeys to sleep overnight. Parents should be encouraged to participate as a lot as attainable within the care of their youngster. Each bed area should be standardized so that it can be used to present any degree of care. While the fetus lives in a low oxygen setting, the oxygen content of the blood of the fetus is similar to that of adults (20 mL of oxygen per a hundred mL of blood) because of the next concentration of hemoglobin that has excessive affinity for oxygen. The neonatal circulation has a number of shunts-the ductus arteriosus, ductus venosus, and foramen ovale-that direct extra oxygenated blood to the brain and heart and bypass the lungs. Changes then happen that enable parallel circulation of the fetus to convert to the sequence circulation of the grownup: 1. This exposes the ductus to oxygenated systemic arterial blood, which along with the rapid decrease in prostaglandin E2 after start, closes the ductus. The ductus venosus closes passively with removing of the placental circulation and readjustment of portal pressure relative to inferior vena cava stress. During fetal life, the central pulmonary vascular mattress has a comparatively thick muscle layer. After birth, the muscle coat thins and extends to the periphery of the lung, a course of that takes months to years to full. The latter embrace obstructive lesions of the left facet of the center (mitral valve stenosis, aortic valve stenosis, aortic stenosis, anomalous pulmonary venous return, ventricular septal defect, or patent ductus arteriosus with a right-to-left shunt), whereas hypoxic lesions embody tricuspid valve stenosis, pulmonary valve stenosis, pulmonary artery stenosis or aplasia, and the tetralogy of Fallot. The fetal coronary heart has lowered catecholamine shops and increased sensitivity to exogenously administered norepinephrine. Human newborns have low cardiac shops of norepinephrine and decreased numbers of sympathetic nerves after delivery. In human neonates, the cholinergic system is totally developed at birth, and the guts is sensitive to vagal stimulation. In preterm infants, postural modifications elicit no change in heart price, suggesting an incomplete or attenuated baroreceptor response. The fetal bradycardia that happens in response to hypoxia is thought to be mediated via chemoreceptors and may be much like the oxygen-conserving mechanisms of diving animals. Relative hypoxia is normal in utero, and infant hearts tolerate hypoxia better than adult hearts do. This difference could additionally be due partially to excessive concentrations of glycogen in fetal myocardial tissue and to the ability to use anaerobic metabolism extra successfully. Because of the high glycogen shops and the ability to use anaerobic metabolism effectively, the fetal or newborn heart is comparatively resistant to hypoxia and may be resuscitated more simply if oxygenation and perfusion are reestablished reasonably rapidly. Cyanotic congenital heart lesions � Tetralogy of Fallot � Transposition of the great arteries � Hypoplastic left heart syndrome � Pulmonary atresia with an intact ventricular septum � Single ventricle � Total anomalous pulmonary venous return � Tricuspid atresia 2. Cardiac catheterization is often carried out as interventional therapy or as a diagnostic device. The ductus arteriosus have to be maintained open in instances of hypoplastic left heart syndrome, aortic stenosis or atresia, interrupted aortic arch, and symptomatic neonatal coarctation of the aorta. In many circumstances, infusion of prostaglandin E1 sustains life till surgical palliation could be performed. Classification of Shock There are a number of schemas that clinicians use to classify shock. Furthermore, within these classification schemas, illness states can fall into a couple of category. One classification schema separates shock into hypovolemic, cardiogenic, distributive or vasogenic, and extracardiac obstructive.