Co-Amoxiclav dosages:
Co-Amoxiclav packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills
Purchase co-amoxiclav online now
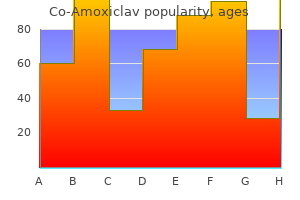
Why do colors seem totally different under fluorescent gentle versus incandescent lights Tungsten (incandescent) gentle bulbs emit relatively extra photons of the longer (red) wavelengths than of the shorter (blue) wavelengths, whereas fluorescent light bulbs emit relatively extra light in the blue and green wavelengths. A shopper who picks out materials for drapes in a store that has fluorescent lighting may be stunned to search out out that the fabric seems fairly different at home. A purple costume appears redder under incandescent gentle than it does under fluorescent gentle. Rods operate finest within the dark-adapted state and cones operate in the light-adapted state. Any color may be produced by overlapping red, green, and blue lights within the correct proportions. On Earth, the atmosphere, which incorporates ozone, mud, water droplets, and tons of different reflecting molecules and substances, is interposed between the solar and our eyes. Therefore, if in the course of the daytime we look away from the solar, we see the blue photons which may be being bent toward us and the sky seems to be blue. Therefore, much more of the blue and green photons are bent away from the environment. If some of these are ultimately reflected towards us by clouds or dust, we see a pink sky. They have all three completely different kinds of cones, regular focus of the cone pigments, and normal retinal wiring. In dichromats, the cones themselves are regular, however one of many three accommodates the incorrect pigment. For example, in deuteranopes, the ``G' cones are regular in each method besides that they contain erythrolabe (red pigment) as an alternative of chlorolabe (green pigment). In protanopes, the ``R' cones are regular in each method besides that they contain chlorolabe (green pigment) as a substitute of erythrolabe (red pigment). In deuteranopia, as a result of each R and G cones include the same pigment, when red mild strikes the retina, the R and G cones are stimulated equally and ship an equal variety of messages to the R-G middle. In different words, the hue heart thinks that equal portions of pink and green gentle are striking the retina. When green or blue-green mild strikes the retina, the R and G cones are once more stimulated equally. In anomalous trichromatism, two of the three cone pigments are normal, however the third capabilities suboptimally. Depending on which pigment is abnormal, the affected persons are termed protanomalous, deuteranomalous, or tritanomalous. Anomalous trichromats can distinguish between totally saturated colours but have issue distinguishing colors of low saturation (pastels) or low luminance (dark colors), or both. Deuteranomaly is present in roughly 5% of the population; deuteranopia, protanopia, and protanomaly in 1% each; and tritanopia or tritanomaly in only 0. In different words, the ladies have completely normal color imaginative and prescient, however approximately 50% of their sons are abnormal. Both men and women can have the tritan issues, that are inherited as autosomal dominant traits (Table 4-1). As a very common rule, the errors made by persons with optic nerve disease are inclined to resemble these made by protans and deutans, whereas these made by individuals with retinal illness resemble these made by tritans. This response occurs secondary to transretinal motion of ions induced by the light stimulus. This is called Ganzfeld or full-field stimulation, which is achieved with a bowl perimeter. The light-induced electrical discharges are recorded from the attention with a corneal contact lens electrode. The constructive b wave following the a wave is generated by the Muller cells and bipolar cells in � the outer retina. Oscillatory potentials are small wavelets which might be superimposed on the b wave and arise from cells in the midretinal layers. Under certain recording situations, additional waveforms may be famous, such as the c wave following the b wave, which displays electrical exercise on the stage of the retinal pigment epithelium and is recorded within the dark-adapted eye. The amplitude (in microvolts) of the a wave is measured from baseline to the trough of the a wave, and the b wave amplitude is measured from the trough of the a wave to peak of the b wave. The implicit time (in milliseconds) is the time from the stimulus onset to peak of the response. The implicit time is measured from the stimulus onset to the peak of the a wave (1) or b wave (2).
Purchase co-amoxiclav 625mg without prescription
Systolic time intervals and echocardiograms have been used to detect cardiotoxicity earlier than the incidence of clinically significant damage. In animals, approximately 50% of an injected dose is excreted unchanged in bile and 10% i n urine. Clinical Uses an important clinical use of dactinomycin is the therapy of Wilms tumor in children and of rhabdomyosarcoma. Occasionally, this drug is used to inhibit immunologic responses associated with organ transplantation. Side Effects the poisonous effects of dactinomycin include the early onset of nausea and vomiting, usually followed by myelosuppression manifesting as pancytopenia 1 t o 7 d ays after completion of remedy. Pancytopenia could also be preceded by thrombocytopenia as the primary manifestation of bone marrow suppression. Glossitis, ulcerations of the oral mucosa, diarrhea, alopecia, and cutaneous erythema are commonly associated with dactinomycin therapy. The drug accumulates in tumors, suggesting the presence of a decrease level of inactivating enzyme. Bleomycin is eradicated primarily by renal excretion, with roughly 50% o f the dose cleared within four hours and 70% by 24 hours. Clinical Uses Bleomycin is efficient in the therapy of testicular carcinoma, particularly if administered together with vinblastine. It can also be useful within the palliative remedy of squamous cell carcinomas of the pinnacle, neck, esophagus, skin, and genitourinary tract. Side Effects the commonest side effects of bleomycin are mucocutaneous reactions, together with stomatitis, alopecia, pruritus, erythema, and hyperpigmentation, which occur in roughly 45% of sufferers. The likely mechanism is the release of an endogenous pyrogen, presumably from destroyed tumor cells. An initial small take a look at dose of bleomycin is really helpful to reduce the prevalence of this syndrome. Pulmonary Toxicity probably the most serious side effect of bleomycin is dose-related pulmonary toxicity. Initially, bleomycin produces pulmonary capillary endothelial damage, progressing to alveolar epithelial harm with necrosis of kind 1 and proliferation of kind 2 alveolar cells. It is estimated that some type of pulmonary toxicity (most typically pulmonary fibrosis) occurs in 4% o f sufferers handled with bleomycin. Fatal pulmonary toxicity has occurred with bleomycin doses as little as one hundred mg but more usually within the presence of other danger components (Table 42-3). A delicate form of pulmonary toxicity is characterized by exertional dyspnea and a traditional resting Pao 2. A extra severe type of arterial hypoxemia at rest is associated with radiographic fi dings of interstitial pneumonitis and fibrosis. Lesions are found more regularly in decrease lobes and subpleural areas, and radiographs of the chest usually reveal basilar and perihilar infiltrates. The alveolar� arterial gradient for oxygen is increased, and pulmonary diffusion capacity could additionally be decreased. Pulmonary perform studies have been of no higher worth than medical indicators in detecting the onset of pulmonary toxicity. Early reports of postoperative respiratory failure in bleomycin-treated sufferers instructed that either arterial hyperoxia or excessive crystalloid administration performed a role within the exacerbation of pulmonary fibrosis. For this Table 42-3 Risk Factors for Development of Chemotherapy-Induced Pulmonary Toxicity Total drug dose Age Concurrent or prior chest radiation Oxygen remedy Combination chemotherapy Preexisting pulmonary disease Genetic predisposition Cigarette smoking ( Animal model literature confirms that the continuous administration of inspired oxygen concentrations of higher than 30% i mmediately after exposure to bleomycin increases pulmonary harm. Patients with prior exposure to bleomycin however with no risk components appear to be at a minimal risk from hyperoxia. In distinction, those sufferers with one or more main danger components (preexisting pulmonary damage from bleomycin, which is extra probably if the whole dose is greater than 450 mg; renal dysfunction, which slows clearance of the drug from the lungs; and/ or prior exposure to bleomycin within a 1- t o 2-month period) could additionally be at higher risk for the event of bleomycin-induced hyperoxic pulmonary damage in the operating room. It could also be prudent to take care of these sufferers on the minimum impressed oxygen concentration that can be utilized safely intraoperatively to supply oxygen saturations of larger than 90% by pulse oximetry. The function of excessive crystalloid administration has not obtained the same scrutiny as elevated delivered oxygen concentrations. Accumulation of interstitial fluid may reflect impaired lymphatic operate attributable to bleomycin-induced fibrotic modifications in the lungs. In the future, bleomycin may be changed with phleomycin, an analogue of bleomycin that has lower pulmonary toxicity and a broader effectiveness in opposition to a quantity of kinds of tumors. Vinca Alkaloids Vinca alkaloids characterize the active medicinal components from the pink periwinkle plant and embrace vincristine, vinblastine, vinorelbine, and vindesine.
Discount co-amoxiclav 625 mg visa
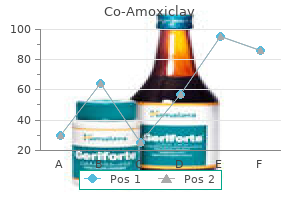
In the hepatocyte part, dysplastic nodules which have retained the flexibility to take up the agent but not to excrete it seem hyperintense due to intracellular cholestasis, whereas nodules which have misplaced the flexibility to take up the agent are hypointense. Geographical morphological traits and isointensity on delayed venous-phase images favor the diagnosis of vascular nontumoral change. Similar to liver tumor, the intravascular mass enhances in the arterial section after contrast injection. The imaging analysis is based on lesion hyperenhancement on late hepatic arterial pictures and depending upon lesion size, different options, including washout on venous/delayed phase pictures, late capsule or pseudocapsule enhancement, and lesion development. Limitations embrace picture degradation by movement artifact and problem detecting and assessing severity of strictures. Because occult cholangiocarcinoma is present in 10% of the resected liver specimens of sufferers with major sclerosing cholangitis,forty two biopsy of suspicious narrowed areas ought to be thought-about before transplantation. Arteriography is carried out when suspected vascular issues are detected on ultrasound studies or in difficult circumstances. With fluoroscopic steering, a specially designed needle-catheter system is used to create a channel from the hepatic vein by way of the hepatic parenchyma to the portal vein. Various stents are used, together with bare steel and polytetrafluoroethylene-covered stents, which have been proven to have greater patency charges. In the immediate postoperative interval, chest radiographs are obtained daily to consider for atelectasis, pneumonia, diaphragmatic paralysis, and pleural effusions. Doppler ultrasonography is the preliminary imaging modality for gross evaluation of the liver parenchyma, biliary tree, and vasculature. Ultrasonography Ultrasonography has an important function in the postoperative monitoring of the liver transplantation affected person. The ultrasound examination ought to include gray-scale ultrasonography of liver homogeneity, bile duct caliber, and the presence of perihepatic and intra-abdominal fluid collections. Perihepatic and intra-abdominal fluid is common within the first postoperative days and steadily disappears. Focal low-attenuation regions of liver parenchyma may represent infarction and prompt more careful evaluation of the hepatic artery branches. Normal Doppler ultrasonography research outcomes might point out a nonvascular reason for graft dysfunction. A full examination ought to embody demonstration of move throughout the hepatic artery proximal and distal to the anastomosis and in each the best and left hepatic arteries. In some cases a high-impedance sample with low or absent move or diastole has been famous early in the postoperative interval, with later return to a extra regular appearance. In patients with the cava interposition anastomosis, the infrahepatic portion is usually readily identifiable, but the suprahepatic anastomosis may be harder to see. Close to the center, a waveform sample just like that of the hepatic veins is seen. A triphasic waveform could be seen in the piggyback anastomosis, reflecting the transmission of pressure modifications from the right heart. Radionuclide research are carried out in liver transplant recipients, primarily within the posttransplant period. A, Doppler ultrasonography velocity profile at the website of the stenosis reveals a high-velocity jet with spectral broadening, indicating turbulence. B, Doppler ultrasonography research of a vessel distal to the stenosis exhibits a dampened irregular waveform with a high diastolic circulate. These compounds are transported from plasma to the hepatocyte by the same transport mechanism as that for bilirubin. Radionuclide analysis is used to assess the functional standing of the graft and to determine structural complications similar to infarcts, abscesses, and bile leaks. In addition to serial radionuclide photographs, time-activity curves are generated for areas of interest such as over the graft and in the left ventricular blood pool. Vascular compromise could happen in the immediate transplant period on the hepatic artery, portal vein, or hepatic vein anastomoses. Hepatic Artery Complications Complications occurring on the site of arterial revascularization include stenosis, thrombosis, pseudoaneurysm, and hepatic artery rupture.
Co-amoxiclav 625mg without a prescription
Versatility and viability of hepatic venoplasty in stay donor liver transplantation using the proper lobe with the center hepatic vein. Reconstruction of double hepatic arterial and portal venous branches for right-lobe living donor liver transplantation. The use of recipient superficial femoral vein as a venous graft for portal vein reconstruction in proper lobe dwelling donor liver transplantation. Surgical procedures for administration of right portal venous branching in right lobe dwelling donor liver transplantation. Life made easy: simplifying reconstruction for twin portal veins in adult right lobe stay donor liver transplantation. Preliminary research of the anatomy of the venous drainage of the intrahepatic and extrahepatic bile ducts and its relevance to the practice of hepatobiliary surgical procedure. Histidine-tryptophanketoglutarate versus University of Wisconsin solution in dwelling donor liver transplantation: outcomes of a prospective research. The introduction of microvascular surgery to hepatic artery reconstruction in living-donor liver transplantation-its surgical benefits in contrast with standard procedures. Microvascular reconstruction of the hepatic artery in live donor liver transplantation: expertise throughout a decade. Flowmetry-based portal influx manipulation for a small-for-size liver graft in a recipient with spontaneous splenorenal shunt. Increasing the recipient benefit/ donor danger ratio by lowering the graft measurement requirement for living donor liver transplantation. Caudal shifting of hepatic vein anastomosis in right liver dwelling donor liver transplantation. Internal hernia of the small bowel after right-lobe reside donor liver transplantation. Biliary reconstruction and problems of right lobe live donor liver transplantation. Abdominal drainage after hepatic resection is contraindicated in sufferers with chronic liver illnesses. Because of the overwhelming scarcity of liver grafts from deceased donors to meet the demand, the variety of grownup dwelling donor liver transplantation has increased dramatically all through the world. In 2008 at Istanbul the Transplantation Society issued a declaration stating that "the availability of care for dwelling donors earlier than, throughout, and after surgery-as described within the stories of the worldwide forums organized by the Transplantation Society in Amsterdam and Vancouver-is no much less important than taking care of the transplant recipient," and that "a optimistic end result for a recipient can by no means justify hurt to a reside donor. It is also extraordinarily important to affirm donor understanding of the dangers and advantages concomitant to the process and that she or he is making an autonomous and noncoerced decision. An intricate steadiness of defending the donor by performing the smallest resection potential and at the similar time providing the recipient with sufficient liver mass and greatest probability for survival has to be sought. The smallest resection that would provide enough useful mass for the recipient can solely be called appropriate. When a nonright liver graft meets the first two criteria, a proper liver graft should, in general, not be selected. A proper lateral sector graft ought to be chosen when the estimated graft volume is bigger than the volume of a left liver with caudate lobe graft and when the right lateral sector graft dimension satisfies the criterion. Left liver with caudate lobe grafting is the standard grafting procedure for the left liver. The transverse portion of the left portal vein runs alongside the right finish of the lesser omentum to the ligamentum venosum, whereas the umbilical portion runs up into the umbilical fissure. The overwhelming majority of donors (more than 90%) have standard anatomy27; nonetheless, about 10% of donors have a trifurcation within the portal venous anatomy during which the proper lateral portal vein branches off independently from the principle portal vein. One in 4 people have their left hepatic artery arising from the left gastric artery. In 7% the left hepatic artery alone branches out from the common hepatic artery due to the changed proper hepatic artery. Accurate recognition of anatomy may even assist in deciding on essentially the most acceptable donor in circumstances the place multiple candidates exist.
Buy cheap co-amoxiclav 625 mg line
Pediatric liver transplantation with cadaveric or dwelling associated donors: comparative ends in ninety elective recipients of primary grafts. Extra-anatomical hepatic artery reconstruction in residing donor liver transplantation: can this process save hepatic grafts? Hepatic artery reconstruction with inferior mesenteric vein graft in pediatric living donor liver transplantation. Biliary reconstruction for infantile living donor liver transplantation: Roux-en-Y hepaticojejunostomy or duct-to-duct choledochocholedochostomy. Biliary reconstruction in pediatric live donor liver transplantation: duct-to-duct or Roux-en-Y hepaticojejunostomy. In fact, roughly 2000 sufferers either die or are removed from the transplant listing as too sick to transplant every year. That is, the potential recipient should full a comprehensive evaluation to make sure that she or he is appropriate for transplantation. Therefore the transplant could also be carried out earlier than the candidate deteriorates to the purpose that the result of the surgery is jeopardized. However, the good thing about an expedited transplant should be balanced with the inherent danger for demise or problems from the surgical procedure itself. However, not all of those sufferers are thought of surgically suitable for the process. These include advanced mesenteric venous thrombosis, a number of medical comorbidities, simultaneous renal transplantation, retransplantation, and others. Large body size is a selected drawback within the United States, the place obesity charges proceed to climb. Although estimates vary on the minimally acceptable weight of a donor organ, the estimated decrease restrict of acceptability is 0. For bigger recipients (whose graft dimension requirements are even higher), most potential donors are just too small to yield an adequately sized graft. In addition, larger donors could also be too overweight to be considered for the donor operation. Consequently, small sufferers are most likely to wait longer and have larger ready listing mortality charges. Most important, the donor has a limited time to undergo evaluation and will not have sufficient time to adequately consider his or her determination to donate. In addition, the transplant team is under stress to carry out a comprehensive, cautious donor analysis over a very short time interval. In addition, the potential donor could learn about the risks and benefits of the operation in order that she or he can make an informed determination relating to donation. The actual risk for death is troublesome to determine due to the low number of donor deaths, as properly as difficulties in identifying donor deaths and their attribution to the operation. Most facilities subsequently evaluate only donor candidates with a big long-term relationship with the recipient who would reasonably incur such a danger. There are uncommon people, deemed "good Samaritan" or altruistic donors, with no emotional ties to the recipient, who willingly undergo the donor operation. The donor analysis is carried out in a staged method to disqualify inappropriate donors as early in the process as potential, thereby minimizing pointless and invasive testing. The course of is started at most facilities with the potential donor contacting the transplant heart to provoke the donor evaluation. One method to initiate the process is for potential donors to contact the center to relate basic info, including age, height, weight, prior surgical procedures, medical issues, medications, marital/family standing, blood type (if known), and cause for donating. Many poor donor candidates could also be disqualified following review of this preliminary information. At most centers donor candidates should be between the ages of 18 and 55, though older donors have successfully donated. Exclusion standards for donor candidates based mostly on their medical and surgical historical past varies by heart. Candidates with lesser stomach operations (appendectomy, ovarian cystectomy) are usually thought of suitable. Any medical problem that may jeopardize the well being or success of the donor operation is exclusionary. Such issues embrace diabetes, important cardiac history, current historical past of noncutaneous malignancy, and others. The donor should be approximately 70% of the load of the recipient to yield a sufficiently massive graft (see earlier discussion).
Order co-amoxiclav 625 mg online
These medication may be categorized into tertiary amines, which inhibit reuptake of each serotonin and norepinephrine (amitriptyline, imipramine, clomipramine) and secondary amines, that are primarily norepinephrine reuptake inhibitors (desipramine, nortriptyline). Despite the immediate onset of this effect, the development of a therapeutic antidepressant impact is inexplicably delayed for 2 t o 3 w eeks. Furthermore, some medication with out results on uptake of biogenic amines are effective antidepressants. It appears likely that potentiation of monoaminergic neurotransmission in the mind is only an early event in a fancy cascade of occasions that finally results in an antidepressant effect. Indeed, chronic administration of those medication is related to (a) decreased sensitivity of postsynaptic b1 and serotonin2 receptors and of presynaptic a2 receptors, and (b) elevated sensitivity of postsynaptic a1 receptors. Pharmacokinetics Tricyclic antidepressants are effectively absorbed from the gastrointestinal tract after oral administration, reflecting high lipid solubility. Therapeutic plasma concentrations (parent drug plus the pharmacologically active demethylated metabolites) are 100 t o 300 ng/ mL, whereas toxicity is in all probability going at ranges greater than 500 ng/mL. Tricyclic antidepressants are strongly certain to plasma and tissue proteins, which, in combination with high lipid solubility, results in a big quantity of distribution (up to 50 L/kg) for these drugs. The long elimination half-time (17 to 30 hours) and wide selection of therapeutic plasma concentrations make once-daily dosing intervals eff ctive. Metabolism Tricyclic antidepressants are oxidized by microsomal enzymes in the liver with subsequent conjugation with glucuronic acid. The particular person variation in fee of metabolism Chapter forty three � Drugs Used for Psychopharmacologic Therapy 827 between patients is 10- to 30-fold. The elimination of tricyclic antidepressants happens over several days, with 1 week or longer required for excretion. Both these lively compounds are inactivated by oxidation of hydroxy metabolites and by conjugation with glucuronic acid. Nortriptyline, which is the pharmacologically active demethylated metabolite of imipramine and amitriptyline, can accumulate to levels that exceed the precursors. Doxepin additionally appears to be transformed to an lively metabolite, nordoxepin, by demethylation. Individual variation within the incidence and type of unwanted effects could additionally be related to the plasma concentrations of the tricyclic antidepressant and its active metabolites. Anticholinergic Effects the anticholinergic effects of tricyclic antidepressants are outstanding, especially at high doses. Amitriptyline causes the highest incidence of anticholinergic results (dry mouth, blurred imaginative and prescient, tachycardia, urinary retention, slowed gastric emptying, ileus), whereas desipramine produces the fewest such effects (see Table 43-2). Anticholinergic delirium may occur in elderly patients even at therapeutic doses of those drugs. Serious anticholinergic toxicity may mirror the results of polypharmacy with more than one anticholinergic drug (over-the-counter preparations to treat diarrhea or insomnia). Elderly sufferers have larger sensitivity to anticholinergic and different receptor results compared with younger patients being handled with tricyclic antidepressants. Cardiovascular Effects Orthostatic hypotension and modest will increase in coronary heart rate are the commonest cardiovascular unwanted effects of tricyclic antidepressants, presumably refl cting druginduced inhibition of norepinephrine reuptake into presynaptic nerve terminals. The threat of hypotension throughout general anesthesia in sufferers treated with tricyclic antidepressants is low however has been reported. Direct cardiac depressant results might mirror quinidinelike actions of tricyclic antidepressants on the guts. Conceivably, there is also enhancement of depressant cardiac effects of anesthetics by tricyclic antidepressants. Quinidine-like properties of tricyclic antidepressants are thought to mirror slowing of sodium ion flux into cells, resulting in altered repolarization and conduction of cardiac impulses. Central Nervous System Effects Sedation associated with tricyclic antidepressant therapy may be desirable for administration of depressed sufferers with insomnia. Amitriptyline and doxepin produce the greatest diploma of sedation (see Table 43-2).
Proven co-amoxiclav 625 mg
The pathological condition of the liver will depend on the diagnosis and indication for liver transplantation. Genetic causes could affect greater than only one main organ; an example is amyloidosis, with which vital cardiac amyloidosis may occur. Hepatocellular cancers might develop especially within the presence of chronic viral hepatitis. It may be characterized by adjustments in mental standing and fluctuating neurological signs-asterixis and hyperreflexia. This permits the accumulation of poisons similar to ammonia, mercaptans, short-chain fatty acids, and phenol, inflicting deleterious effects on the brain. The failure of the liver to convert ammonia to urea ends in the buildup of ammonia, which exacerbates the encephalopathy. The liver is also answerable for the formation of plasma proteins aside from immunoglobulins. This contains not only the coagulation factors but additionally albumin, which is responsible for sustaining a standard plasma oncotic strain and in addition the transport of a selection of medication. Therefore a discount in serum albumin stage will permit edema formation and also a rise in the unbound fraction of many drugs. However, because of the danger for bleeding in this affected person population, many neurosurgeons defer placement of the monitor. An aggressive correction of the coagulopathy is required before the location of a monitoring system. Brain monitoring with electroencephalography and the electroencephalogram-derived bispectral index throughout cardiac surgical procedure. Very small modifications in hemodynamics could cause main modifications in cerebral perfusion stress. The use of cerebral perform screens that display the cortical electrical exercise of the mind could also be useful adjuncts in management. The prevention of quantity overload and the rise in central venous pressure may be facilitated by the early introduction of steady venovenous hemodialysis. This is necessary to know as a end result of extreme cardiomyopathy is incessantly associated with liver cirrhosis. Similarly, as a outcome of this is a highcardiac output cardiomyopathy, reperfusion of the liver graft on the time of transplantation, which usually ends in a further acute enhance in cardiac output, might precipitate ventricular dysfunction, both right and left, causing graft dysfunction. The examination by echocardiography could initially be interpreted as regular cardiac operate due to the significant discount in afterload brought on by the low systemic vascular resistance. However, on nearer examination both systolic and diastolic dysfunction may be demonstrated. Any affected person who presents for liver transplantation and is found to have a low cardiac index and elevated filling pressures must be intently examined for the presence of a cardiomyopathy. However, the most typical cause of a low cardiac index in the immediate preoperative period is hypovolemia. The cirrhotic cardiomyopathy does enhance after liver transplantation with disappearance of diastolic dysfunction and normalization of the cardiac response to stress. If the coronary arterial obstructive lesions may be dilated and a bare-metal stent positioned, liver transplantation could also be an acceptable-risk procedure. Conversely, the unavoidable major hemodynamic adjustments that will occur throughout liver transplantation make this selection very hazardous if it is undertaken first. This therapeutic dilemma requires shut consultation among the many heart specialist, anesthesiologist, and surgeon. Plotkin et al36 demonstrated that the dobutamine stress echocardiogram had a sensitivity of one hundred pc, a specificity of 90%, a constructive predictive value of 100%, and a negative predictive worth of one hundred pc when evaluating liver transplant candidates with cardiac danger elements. The mixture of a cirrhotic cardiomyopathy and the administration of -blockers can make catecholamine responses very blunted during liver transplantation. The monitoring of the cardiovascular system should embody intra-arterial and central venous pressure sensors.
Generic co-amoxiclav 625mg overnight delivery
Intravascular entry catheters are the most typical causes of bacteremia or fungemia in hospitalized sufferers. Special Patient Groups Parturients Administration of antimicrobials during pregnancy introduces the question of safety for the mom and fetus (Table 41-5). Increases in maternal blood quantity, glomerular filtration rate, and hepatic metabolic exercise could decrease plasma antimicrobial concentrations (10% to 50%), particularly late in pregnancy and in the early postpartum period. In some parturients, delayed gastric emptying might lower absorption of orally administered antimicrobials. Conversely, administration of aminoglycosides and vancomycin to elderly patients could require adjustments in dosing regimens. Measurement of plasma concentrations of antimicrobials and monitoring of renal function could also be indicated when administering certain antimicrobials to elderly sufferers. Several recent studies have addressed this concern and produced conflicting results. The penicillins may be classified into subgroups because of their construction, b-lactamase susceptibility, and spectrum of activity. Penicillins additionally lower the availability of an inhibitor of murein hydrolase such that the uninhibited enzyme can then destroy (lyse) the structural integrity of bacterial cell walls. Cell membranes of resistant gram-negative bacteria are generally resistant to penicillins because they prevent access to websites the place synthesis of peptidoglycan is happening. Clinical Indications Penicillin is the drug of choice for treatment of pneumococcal, streptococcal, and meningococcal infections. Gono- cocci have gradually turn out to be more immune to penicillin, requiring greater doses for adequate remedy. Penicillin is the drug of choice for treating all forms of actinomycosis and clostridial infections inflicting gas gangrene. Transient bacteremia occurs within the majority of sufferers present process dental extractions, emphasizing the importance of prophylactic penicillin in sufferers with congenital or acquired coronary heart disease or tissue implants present process dental procedures. Transient bacteremia may also accompany surgical Chapter 41 � Antimicrobials, Antiseptics, Disinfectants, and Management of Perioperative Infection 791 procedures, corresponding to tonsillectomy and operations on the genitourinary and gastrointestinal tracts, and vaginal supply. If this amount of potassium introduces a threat to the patient, a sodium salt of penicillin G or a sodium salt of a similar penicillin, similar to ampicillin or carbenicillin, could be substituted for the aqueous penicillin G. Furthermore, arachnoiditis and encephalopathy may observe intrathecal penicillin administration. Approximately 10% is eradicated by glomerular filtration, and 90% is eradicated by renal tubular secretion. Duration of Action Methods to delay the length of motion of penicillin embrace the simultaneous administration of probenecid, which blocks the renal tubular secretion of penicillin. Procaine penicillin accommodates a hundred and twenty mg of the native anesthetic for each 300,000 U of the antimicrobial. Possible hypersensitivity to procaine have to be thought-about when deciding on this form of the antimicrobial for administration. Oxacillin and nafcillin, unlike methicillin, are comparatively secure in an acidic medium, leading to enough systemic absorption after oral administration. Cloxacillin and dicloxacillin are available only as oral preparations and could additionally be preferable as a result of they produce higher blood levels than do oxacillin and nafcillin. They are, nonetheless, all inactivated by penicillinase produced by sure gram-negative and gram-positive bacteria. Ampicillin Ampicillin (a-aminobenzylpenicillin) has a broader range of exercise than penicillin G. Its spectrum encompasses not only pneumococci, meningococci, gonococci, and numerous streptococci but additionally numerous gram-negative bacilli, such as Haemophilus infl enzae and Escherichia coli. Ampicillin is secure in acid and thus is nicely absorbed after oral administration, though peak plasma concentrations are decrease than these achieved after administration of penicillin V. Approximately 50% of an oral dose of ampicillin is excreted unchanged by the kidneys in the first 6 h ours, emphasizing that renal perform significantly influences the duration of action of this antimicrobial. Among the penicillins, ampicillin is associated with the best incidence of skin rash (9%), which typically appears 7 to 10 days after initiation of therapy. Specific indications for these medicine are infections brought on by staphylococci known to produce this enzyme.